Four Ways HEOR Data Paves the Way to DTx Commercial Success
The Fall and Rise of Digital Therapeutics
Decentralized Clinical Trials: Bust or Breakthrough?
Decentralized to Digital, A Pioneer Engages Big Pharma
Industry Leaders Discuss the Impact of FDA's Diversity Action Plan
Pharma Pulse 7/3/24: Reactions to New FDA Diversity Action Plan Guidance, Walgreens Strengthens Support for Children and Adults Living with Diabetes & more
Status Check: Science & Sustainability
Curavit's new services uncover economic insights and determine therapeutic value
Inspiration from The Sound of Music's von Trapp family influenced this week's woman in science
Japan's success in digital health is attributed to the collaborative efforts between the government, private sector, and academic institutions
Is Japan Leading a New Digital Health Movement?
Opinion: Biopharma Should Prioritize Research on the Economics of Therapies
A host of pharma industry experts discuss the increasing use of digital technology in decentralized clinical trials
Digital Therapeutics Find Opportunity in Healthcare Economics Outcomes
Changing the Face—and Faces—of Clinical Research
Drop the “D” - Experts consider how decentralized clinical trials will change in the future
Sana strives for breakthrough designation as VR PTSD trial concludes
Digital Therapeutics: The Promise of Virtual Reality Masks in Treating PTSD Symptoms
Attending SCOPE - important to understand the latest trends in clinical research
Predictions for the Life Sciences 2024: Science and Technology
PharmaVoice’s Crystal Ball: What’s next in drug innovation and clinical trials
Understanding the Value of Mergers and Acquisitions in Life Sciences
Pharma IT and AI – 2024 Health IT Predictions
DCTs, Digital Therapeutics to Make Further Headway in 2024, Say Experts
Evaluating the Oncology Landscape: Diagnosis, Treatment, Predictions
Media Coverage | Pharmaceutical Commerce
How Healthcare Economics Outcomes Evidence Can Pave the Way for Digital Therapeutics
Why digital therapeutics (DTx) are effective and safe, but not being prescribed
A Look Back at Diversity, Equity & Inclusion in 2023
PM360 2023 Innovative Clinical Trial Curavit Clinical Research’s Central Virtual Site
Diversity and ePROs: Still siloed concepts in the era of DCTs?
Life sciences industry predictions 2024: Curavit
The digital therapeutics revolution is here. Will payers play ball?
Podcast: Discussing The Potentials Of And Challenges For Digital Therapeutics
Digital Therapeutic Clinical Trials: A Pioneering Approach to Better Treatments
A New Tool for Helping Labs Improve Diversity in Clinical Trials
Curavit capturing health economics evidence with new HEOR practice
New FDA Regulations for Diversity and Inclusion in Clinical Trials for 2024
How Companies Are Upping Diversity Among Clinical Trial Participants
Clinical Trial Inclusivity, Diversity, and Equity in Action
Women in Health: Curious, Persistent, Resilient: Natalia Husby, CluePoints
Curavit Chosen as Contract Research Organization for MedRhythms Clinical Trial
MedRhythms sounds out Curavit to study auditory stimulation tech on stroke patients
Curavit VCRO chosen to manage study of MedRhythm's neurorehabilitation system for stroke patients
Decentralized Clinical Trial Platform Secures Study---Growth in Changing Market
MedRhythms Selects Curavit for MR-001 Trial in Stroke Impairment
Improving Health Equity and Diversity Throughout the Life Sciences
Rigorous Data Are Key to Convince Payers, Investors in the World of Digital Therapeutics
Wall Street Journal Pro
Curavit: Tackling under representation with the right balance of patient care, science and business
Slice of Health Care | Podcast Episode
A Crossroads for the Digital Therapeutics Industry. Now is the Time to Act
Contract Pharma - CRO Industry Market Report
Finding a balance: Blending traditional and digital clinical trials for DTx
Banging Down Doors to Breaking Glass Ceilings: Better Health Equity for Women
Twists and Turns on the Winding Road of Digital Therapeutics: From Product Development to Approval to Access
Swing Therapeutics’ Approach to the DTx Market Access Problem and Clinical Trial Recruitment
Making Clinical Trials Better for Everyone in 2023
Why Three Doctors are in Favor of Decentralized Clinical Trials
Digital therapeutics 2023: Swing and trial partner Curavit kick off fibromyalgia study
Virtual Site Brings Speed, Diversity, And Engagement To Digital Therapeutic Trial
Industry Predictions For 2023
Curavit’s crystal ball – how will 2023 drive meaningful changes in clinical research
Digital Therapeutics: From Product Development and Approval to Commercialization and Reimbursement
Virtual CRO Curavit raises $5m to grow digital therapeutics clinical trial business
Can pharma prop up the digital health recession?
Curavit Clinical Research Raises $5 Million led by Osage Venture Partners
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Curavit reaps $5M in series A funding to fuel decentralized trial growth
Curavit reaps $5M in series A funding to fuel decentralized trial growth
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Curavit Clinical Research raised $5 million in Series A funding
More Than One Way to Crack a Walnut: Four Fundamental Components of a Successful Decentralized Clinical Trial
Tips for tackling trial recruitment and retention woes in oncology
Curavit partners with 1nHealth for digital first recruiting of DCT
What’s your leadership brand?
Taking a Virtual Approach to Clinical Trials
ixlayer Partners With Curavit
DE&I Champions: Dr. Pam Diamond
Curavit, Swing team up on fibromyalgia therapeutic trial
For Digital Therapeutics, Virtual Trials Leverage Efficiencies
Video: The State of Decentralized Clinical Trials | Interview
Video: How Can Pharma Improve Clinical Trials?
Unique Considerations in Designing Decentralized Trials for Digital Therapeutics
Digital Therapeutics Deliver Surprising New Benefits for Cancer Patients
Invest in Technology, Profit in Better Health Outcomes
Decentralized Trials Begin to Show Their Value in New Ways
Digital Therapeutics Companies Lean into Decentralized Clinical Trials
Despite rapid DCT evolution, there’s still room for progress: Curavit
Gaining real-world results from a decentralized trial
Home is where the trial is
Oncology: Surprising Therapeutic Area Ripe for Decentralized Research
Digital Therapeutics Sector Projected to Grow Exponentially
Curavit Earns HIPAA Seal of Compliance
PM360 Presents the 2021 Innovators
Advantages of Digital Decentralized Trials with Curavit’s Dave Hanaman | Interview
20 Years in the Making: Reflections and Predictions
Curavit Clinical Research announced the appointments
Decentralized Clinical Trials: What Therapeutic Areas are Ripe for All-Virtual?
Insights into Defining Decentralized Clinical Trials
Decentralized Clinical Trials Poised to Expand Their Reach
Meet The Disruptors: Dave Hanaman Of Curavit Clinical Research On The Three Things You Need To Shake Up Your Industry
Curavit Clinical Research announced the appointments
Decentralized Trials & Research Alliance Grows, Partnerships in Site Conduct, Trial Diversity, More
Curavit joins decentralized trials group, predicts demand will keep growing
Beech Tree Labs Selects Curavit Clinical Research to Push Toward 100% Virtual Clinical Trials
Chapel Hill startup targets seed funding after working to diversify Novavax Covid-19 vaccine trial
17 Virtual Clinical Trial Providers to Partner up With
Curavit Clinical Research, has been launched to help realise the potential of decentralised clinical trials
Prediction for 2024: AI for patient and healthcare professional engagement is booming but expect stricter rules in 2024.
2024 Prediction Review: In 2024, regulatory bodies intensified their scrutiny of AI applications in healthcare. FDA strengthened its oversight to ensure patient safety and foster innovation. This included initiatives like the Breakthrough Devices Program and the Safer Technologies Program (STeP), which facilitate timely access to life-saving devices by expediting regulatory review.
Prediction for 2024: US federal, state, and private watchdogs will check AI not only for accuracy, but also for fairness and bias.
Prediction for 2024: Data privacy as applied to AI will get serious attention from regulators.
2024 Prediction Review: As seen in the Clearview AI facial recognition lawsuit settlement, companies are using nonconsenting user information to train their systems. There are already legislative proposals to require that AI systems get consent prior to using data for training purposes. The FDA, FTC, FCC, and other agencies will likely continue to expand their purview to protect patient subject privacy.
Prediction for 2024: It will become more important to be able to explain how AI works, source the results, and explain what the AI finds.
Prediction for 2024: Lawsuits will begin to be filed over AI mistakes.
2024 Prediction Review: The legal landscape saw significant activity concerning AI-related errors. Notably, one insurer faced lawsuits alleging the use of an AI model with a 90% error rate to deny care, highlighting the critical need for accuracy and accountability in AI applications. This, in combination with the previously discussed ClearView AI lawsuit and the SafeRent algorithm discrimination lawsuit, demonstrates the emergence of and continuing trend of lawsuits resulting from AI-related errors.
Prediction for 2024: If AI is done legally and compliantly, especially by sales and medical information personnel, trust can be built into the system. While FDA has focused on quality by design, AI lawyers will need to work with sales and medical affairs teams to build trust by design into the systems.
2024 Prediction Review: The DOJ recently updated its “Evaluation of Corporate Programs” guidance to include consideration of AI risks to ensure that use of AI will not result in “deliberate or reckless misuse” that violates criminal laws or the company’s Code of Conduct. The US Department of Health and Human Services recently updated its own compliance plan to establish new agency requirements and guidance for artificial intelligence (AI) governance, innovation, and risk management. The FDA is already looking to crack down on “dishonesty in clinical studies” using artificial intelligence.
Accordingly, multiple agencies are all looking to use AI to ensure continued legal compliance and ethical AI deployment.
Darshan Kulkarni, The Kulkarni Law Firm
The Competitive Pharmaceutical Landscape
Prediction for 2024: The competitive pharmaceutical marketplace will compel increased trial innovation: The pharmaceutical marketplace is more competitive than ever, particularly in the race to be first to market. The first-mover advantage is dramatic, so clinical trial sponsors need to be focused on maximizing every second and not wasting time. Decentralized clinical trial (DCT) methodologies will become part of the standard toolkit, embedded into most trial processes and operational decisions, because sponsors need new ways to collect data reliably and engage with patients in a competitive marketplace. In 2024, the shift to DCT methodologies will be transformative and wholesale, bringing DCT elements into the organization at the portfolio level rather than trial by trial.
2024 Prediction Review: At the start of 2024, there was a lot of discussion about the DCT hype cycle and whether we were over it. I suspect that this comes from people who realized just how resilient and rigorous the effort needed to be to implement DCT change management. Based on our work with clinical trial sponsors (having deployed our DCT platform in nearly 400 decentralized and hybrid clinical trials in 70 countries, serving more than one million patients and research participants globally), those who doubled down on DCT value had breakthrough outcomes this year, including 200% faster enrollment and 50% cost reductions. In fact, a Tufts CSDD study shows that, on average, decentralized trials can achieve net financial benefits from five to 13 times for phase 2 and phase 3 trials, equating to roughly $10M ROI and $39M ROI for an investment of $500K in phase 2 and $1.5M in phase 3 trials, respectively.
Further, the Partnership for Advancing Clinical Trials (PACT) consortium in conjunction with the Tufts Center for the Study of Drug Development (CSDD) has produced compelling results from a new study. In total, 13 clinical trial sponsors and contract research organizations provided robust data on 60 clinical trials that deployed decentralized solutions and found that actual timelines beat planned timelines from first site activated to first patient enrolled, and from first patient to last patient enrolled.
Prediction for 2025: The DCT adoption progress made in 2024 will scale exponentially in 2025 as the standards, processes, and capabilities become firmly embedded in everyday practice. This is especially likely as FDA finalized its guidance for trials with decentralized elements, essentially cementing these technologies in our vernacular while showing government support. Earlier engagement in portfolio design will identify greater opportunity to consistently apply digital tooling and data collection standards across suites of studies, streamlining aggregation and resulting in earlier decision-making. It will also help to automate data flow to harness more digital endpoints with greater precision outcome measures to reduce noise and distortion in signal detection. We will see further growth in master protocol designs with digital endpoints captured in real time to inform in-flight decisions on design pivots and cohort management to accelerate time to results. AI advances are also going to accelerate the transformation. There are opportunities to harness AI agents to relieve, and in places remove, manual tasks that are prone to inconsistency and error. In addition, AI will automate many manual activities such as scan reading, uploads of code, trend spotting, and more, to provide higher integrity outputs and data quality.
Alison Holland, Medable
Data Sharing and Cross-Industry Collaboration
Prediction for 2024: Data sharing and cross-industry collaboration will power the 2024 AI revolution in clinical research. No one company has enough data to drive accurate predictions around a single disease or use case, which is why cross-industry collaboration like we witnessed during the pandemic will be reinvigorated.
2024 Prediction Review: This prediction was challenged by industry-wide portfolio prioritization and cost reductions. While the pandemic demonstrated the power of cross-industry collaboration to achieve ambitious goals, post-pandemic conditions produced financial pressures on biopharma organizations, leading to pipeline restructuring and organizational shifts. Amongst other contributing factors, rising R&D costs, inflation, and investor demands for improved margins have driven a narrower focus on core business areas, limiting resources for data-sharing initiatives. However, with ongoing consolidation by large pharma and therapeutic expansion plans for midsized companies, renewed opportunities may emerge in 2025, as these initiatives will depend on insights derived from shared and diverse data not readily available.
Prediction for 2025: In 2025, cross-industry collaboration and data-sharing opportunities are emerging. These include mining study startup data from over 12,000 sites across 55+ countries to predict study timelines for AI-optimized solutions. While these collaborations offer promise for global study optimization, they will likely involve partnerships between individual organizations rather than large consortia, reflecting the market realities of 2024. Additionally, AI applications in 2025 are expected to focus on reducing repetitive workloads rather than groundbreaking discoveries, such as curing ultrarare cancers. One reason for this shift is the relative ease of sharing and leveraging less sensitive operational data compared to safety and efficacy data, ensuring that AI models are effective within existing data-sharing constraints.
Rohit Nambisan, Lokavant
Decentralized Clinical Trials (DCTs): Evidence versus Hypotheses and New Focus on “How”
2024 Prediction: Evidence will replace hypotheses in DCTs: By the end of 2024, the life sciences industry will replace hypothetical surveys about the impact of decentralized methodologies in clinical research with hard evidence. The Tufts Center for the Study of Drug Development has formed a pre-competitive consortium of more than 50 companies that will collate metrics to understand how decentralization impacts protocol performance such as cycle times, patient recruitment, and retention rates, with the goal to publish its first data set by spring 2024. As we continue to capture evidence of DCT value, we will increasingly adopt a nuanced approach, but this progression will move at the pace of maturity of each DCT innovation.
2024 Prediction Review: New trial data is being added every day and the data continues to be analyzed to uncover exactly which DCT elements contribute to what impact, and whether that impact is universal or more pronounced just in certain types of trials based on populations and indications.
The Partnership for Advancing Clinical Trials (PACT) consortium in conjunction with the Tufts Center for the Study of Drug Development (CSDD) released an initial data set based on 69 studies of which only about 20% were completed. In total, 13 clinical trial sponsors and contract research organizations provided robust data on clinical trials that deployed decentralized solutions and found that actual timelines beat planned timelines from first site activated to first patient enrolled, and from first patient to last patient enrolled. The data on the impact is still incomplete, however, as most of the trials did not complete until this year and many more are slated to have a database lock in 2025.
This initial set also showed that study visits are the most common activity supported by DCT solutions. Specifically, eCOAs are the most deployed DCT solution (80% of trials), while portals, apps for data collection, apps for reminders, and home visits were each used in about half of trials in the first year’s data set.
Prediction for 2025: We will gain a much greater understanding in 2025, and we will have the evidence needed for much broader adoption of DCT elements by the end of 2025. For the past two years, decentralized trials have overcome hurdles that were never addressed during COVID. Did they deliver on the promise of faster trials, better representation, and better participant engagement? Yes, data is emerging which shows that cycle times are typically beating plan timelines and that, when deploying decentralized elements, trials have a lower proportion of white participants and a higher proportion of Asian participants, with other groups also showing a modest increase. Some have referred to this past phase as the “trough of disillusionment.” In 2025, we will emerge out of that phase and into the “slope of enlightenment.” We are overcoming skepticism with evidence and improving technology. Regulators have been removing ambiguity with clear guidance, and more will come from ICH E6 R3 Annex 2. As a result, trials with decentralized elements will be deployed in a much more transparent and thoughtful way, benefiting participants with better representation, improving data, and ultimately bringing treatments to patients more rapidly.
2024 Prediction: The acronym “DCT” will disappear as decentralization becomes the norm: By the end of 2024, the life sciences industry won’t distinguish DCTs from “simple” or “traditional” clinical trials anymore. The acronym DCT will become less of a callout as a distinct type of unique clinical trial. Recent FDA and other global regulatory agency guidances explicitly note that decentralized trials simply need to comply with existing regulations for clinical trials—nothing extraordinary. By the end of 2024, decentralized clinical trials will simply be clinical trials (with certain parts appropriately decentralized), and the impact of this model will be much more prevalent.
2024 Prediction Review: Industry still makes distinctions between various types of trials and calls out trials with DCT elements as separate, but the recently released FDA guidances clearly state that “FDA’s regulatory requirements for investigations of medical products are the same for trials that include decentralized elements and trials that do not include decentralized elements.” In other words, trials with decentralized elements are not expected to perform to a different standard than their traditional counterparts. A quilt of options for clinical trials will be deployed fit-for-purpose—from protocol design (quality by design, pragmatic designs, adaptive designs) to execution with decentralized elements embedded within clinical care depending on the medical product, indication, population, and other unique situations.
Pam Tenaerts, Medable
Diversity in Clinical Research Participation
Prediction for 2024: For 2024 and beyond, the focus on patient diversity in clinical trials will increase. There is far more capacity now to connect with broader patient populations using new digital technologies. Given the convenience of these tools, more patients who become increasingly comfortable with technology will take advantage of digital opportunities to connect to a trial and remain engaged through to the end.
2024 Prediction Review: Aligning this focus and determination to change, in addition to greater commitment to meeting the needs of sites and patients to reduce burden and improve accessibility, certainly progressed during 2024. More companies invested in dedicated roles to raise the inclusion and visibility of the patient voice within their plans.
Prediction for 2025: We will see greater investment in studies designed to enable greater accessibility and in tools that make it possible to meet patients where they prefer to have their care interface (on-site, remote, vacation, pharmacy, etc.). This is the key to improving participant diversity and representation in our trials. There will be significantly greater adoption of digital consent technologies not only to reduce trial participation burden on patients but also to improve patient awareness, comprehension, and understanding of trial activities to optimize participant engagement throughout the trial.
Alison Holland, Medable
Generative AI Coupled with Quantum Computing
Prediction for 2024: Generative AI coupled with quantum computing applied to the sciences: Whether it be novel drug candidates or bioprocess improvement, the impact is now just beginning. When AI is powered by quantum computing, it will accelerate the sciences in ways that are currently difficult or even impossible to imagine.
2024 Prediction Review: We are already seeing the signposts of this prediction come to fruition. AI has been successfully applied to repurposing existing therapeutics, as many are aware. Now a new therapeutic candidate has been identified using AI—an antifibrotic small molecule which went into phase 2 in 2024. Add quantum computing to this advancement, and AI will make even more profound impacts. Already, Google has announced its Willow Chip, which has a performance characterization that is hard to imagine; if only a fraction of that proves true in practice, AI will be forever changed. For 2025, I am doubling down on this prediction and suspect that it may be realized sooner rather than later.
Clark Golestani, C Sensei Group LLC
Market Access Models for Digital Therapeutics (DTx)
Prediction for 2024: Current market acceptance for prescription digital therapeutics (DTx) is low and improvement may take years. Given this, many DTx companies will pivot away from the prescription model and go straight to consumers in 2024.
2024 Prediction Review: Broadly speaking, this prediction was accurate. However, there was little overall clinical trial activity in the DTx space in 2024, both in the consumer and the prescription market segments.
Prediction for 2025: FDA released draft guidance on Prescription Drug Use-Related Software (PDURS) in late 2023, marking a significant step towards integrating digital tools with prescription medications. Throughout 2024, stakeholders in the pharmaceutical and digital health industries actively evaluated and developed strategies to align with this guidance. These efforts are expected to gain momentum in 2025, as companies transition from planning to implementing innovative solutions through digital integration.
Joel Morse, Curavit
Pharmacovigilance Guidelines: Remote Audits and Inspections
Prediction for 2024: With global armed conflicts and geopolitical unrest continuing or even intensifying in 2024, it is likely that regulatory inspections and routine audits will continue in remote mode.
2024 Prediction Review: Predictions regarding the worsening of geopolitical tensions turned out to be correct, and while 2024 data is still being collected, many remote audits and inspections were conducted in 2024. I expect the trend to continue in 2025.
Manoj Swaminathan, VigiServe Foundation
Strengthening Medical Device Regulations
2024 Prediction: It is also reasonable to expect FDA to propose new guidance documents to address burgeoning technologies and enhance the safety and efficacy of digitally enhanced medical devices, particularly in connection with cybersecurity, artificial intelligence, machine learning, and digital health applications, in 2024.
2024 Prediction Review: As anticipated, FDA continued to establish guidelines for software as a medical device, artificial intelligence (AI), and machine learning (ML), throughout 2024. This focus on digital health regulations prioritized safety and efficacy, providing a clearer pathway for innovators while ensuring patient protection.
FDA focused on enhancing the safety and efficacy of digitally enhanced medical devices, particularly in areas such as cybersecurity, AI, ML, and digital health applications. This proactive approach demonstrated the agency’s commitment to keeping pace with rapid technological advancements.
In addition, 2024 saw a significant amalgamation of medical devices with novel digital health technologies, leading to groundbreaking solutions for diagnosis, monitoring, and treatment. This integration has, as predicted, indeed transformed both clinical research and healthcare delivery.
Finally, the increased connectivity of medical devices led FDA to implement fortified cybersecurity regulations to safeguard trial participant privacy and device integrity. This development underscored the growing importance of data security in the medical device landscape.
Isaac R. Rodriguez-Chavez, 4Biosolutions Consulting
Unlike pharmaceuticals (pills and injectables), medical devices come in all different shapes, sizes, forms, and price points—from bandages to robotics and software as a medical device (SaMD). The breathtaking innovation that drives continual shape-shifting in the medical device industry is the same driver of endless change in clinical trials, regulatory review, market access, go-to-market models, formulary acceptance, pricing strategies, and payer reimbursement. SaMD is one of the most novel new medical device products entering the marketplace today, but it has the least clear path to commercialization. These are also often referred to as digital-based medical devices or digital therapeutics (DTx).
DTx have a particularly murky roadmap because there is still no infrastructure in place, and they are not well-understood by clinicians, payers, and patients. For this reason, health economics outcomes research (HEOR) is so important because, put simply, money talks. The companies that incorporate this data capture in their clinical trials conclude their research not only with validation of safety and efficacy but also with the financial impact of the product on the broader healthcare system.
Safety and Efficacy Aren’t Enough
Over the last decade, prescription digital therapies have proven their medical value. Specifically, DTx products have played a significant role in the effective management of a variety of mental health issues, including substance abuse, sleep disorders, depression, ADHD, and others. According to the World Health Organization, nearly 1 billion people worldwide live with a mental health disorder yet three-quarters of these individuals receive no treatment, either because of a lack of access to care or the stigma surrounding their condition.1 Digital therapeutics are closing this gap—providing more and better options, as well as convenient and discreet access to care for those in need.
DTx have also proven effective complementary therapies to traditional drugs to treat chronic conditions, including sleep disorders and pain management. For example, Swing Therapeutics recently completed a phase 3 trial with positive results, leading to FDA approval for Stanza—a self-guided, smartphone-based therapy to treat fibromyalgia, a chronic and debilitating pain condition that affects more than 10 million Americans.2 Stanza provides an easily accessible behavioral therapy option that can be used alongside medication, physical therapy, and other standard-of-care treatments.
“One of the exciting things about new technology as well as one of the challenges is that it really opens up new ways to develop products,” said Mike Rosenbluth, Ph.D., CEO at Swing Therapeutics. “How can we adapt those processes for the new intervention, as many of the processes of developing a drug are not relevant for digital-based medical device products or DTx. So, we’re committed to evidence development and demonstrating that our products are clinically effective—the industry needs to build on a solid foundation of evidence so that digital therapies can be adopted as standard of care.”
Yet, despite DTx effectiveness, healthcare professionals have been slow to prescribe or recommend them to patients. The reasons for this are complex and multifaceted. The lack of widespread knowledge and understanding about DTx products among clinicians, as well as complications with prescribing these therapies, various administrative challenges, and insufficient insurance coverage have all added to the challenges of getting these treatments into the hands of those who they can help.
Clearly, producing safe and effective DTx products that improve outcomes for patients is not enough. The road to viability is longer and more daunting. One solution can be found in the health economic value of DTx products. The more companies can prove both safety and efficacy as well as value, the better opportunities they will ultimately have at improving market access, payer coverage, and clinician and patient adoption.
As healthcare costs continue to rise, payers are concerned with health outcomes and cost-effectiveness. This is particularly so for less-understood digital therapeutics. It’s critical to capture evidence of the value of these innovations, both as it pertains to individual patients in certain therapeutic areas as well as its impact on the broader population.
“Targeted clinical trial, economic, and real-world data will drive adoption of DTx products,” Andy Molnar, CEO of the Digital Therapeutics Alliance, a trade organization focused on the needs of the clinically validated digital therapeutics industry. “Capturing the right data that proves to all stakeholders—government, commercial insurers, medical directors, providers, and patients—to adopt these products, however, is complex. It is even more daunting for DTx startups that may not have the same resources as pharmaceutical companies.”
Case in Point: MedRhythms
MedRhythms, a rapidly growing digital-based medical devices company, recognized the importance of capturing HEOR data from day one. MedRhythms pioneered a neurotherapeutic designed to improve walking, mobility, and related functional outcomes by using a proprietary, patented technology platform that combines sensors, software, and music with advanced neuroscience to target neural circuitry. The company is developing a pipeline of digital therapeutics across a range of neurological conditions, including stroke, multiple sclerosis, and Parkinson’s disease.
The company worked with Curavit to investigate long-term patient adherence, response durability, and healthcare economic value of its novel neurorehabilitation system to improve walking in adults with chronic stroke walking deficits. The study—known as OrcHESTRAS (Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation)3—is a prospectively enrolled study, with a novel design that focuses on evidence generation and exploration of a product’s impact on reducing the financial impact on the U.S. healthcare landscape.
“A cornerstone of our mission is that our products must be accessible to patients. One way we do that is through furthering our evidence development,” said Owen McCarthy, president and co-founder of MedRhythms. “We need to speak the same language as payers in order to gain traction for a new prescription-only product just as much as we need to demonstrate efficacy to providers.”
Four Reasons to Incorporate HEOR in Clinical Research
Market Access for Reimbursement: One of the biggest impediments to commercial acceptance and clinician prescribing of digital-based medical devices is the lack of both private and government reimbursement. However, with HEOR evidence illustrating it can lower an insurer’s overall cost, more patients will gain access to the option.
Regulatory Acceptance: While many products are first approved or cleared for one indication, they have the potential to be used across several indications. However, before they can be used for additional treatments, more evidence is required. MedRhythms’ device is approved for stroke based on a 12-week study but is now involved in a 12-month study to capture more regulatory data and HEOR data. That HEOR and efficacy data captured over a longer period shows durability in existing applications as well as demonstrating the potential for other indications.
Product Development: Since HEOR data is typically captured over months rather than weeks, it provides developers with greater insight into the device’s everyday use over time. How easy is it to use? How easy is it to recharge? These are usability characteristics that wouldn’t necessarily be tracked in a clinical trial, but a longer-term HEOR trial helps to capture more nuanced information about the device to inform future product improvement.
Influence on Reimbursement (at the federal level): HEOR data offers crucial evidence that can impact government policies and federal agencies to help improve the industry overall and pave the way for the adoption of these devices. HEOR demonstrates the economic benefit of digital-based medical devices or DTx as additive/supplemental therapies to existing therapies and drugs. HEOR proves the economic advantages of adding these devices into the therapy regimen as well as their benefits as standalone options.
Save the System
It’s no secret the U.S. healthcare system is hemorrhaging dollars while also failing to provide requisite care for all Americans. Rising costs of labor, drugs, medical supplies, and equipment mean that over the next six years, annual health expenditures in the U.S. are expected to increase from $4 trillion to $8.3 trillion.4 This surge—combined with lower reimbursement rates, financial challenges from the pandemic, and aging infrastructure—means approximately 30% of U.S. rural hospitals are at risk of closure.5 Implications would include reduced access to care, patients traveling further for care, and potential delays in treatment. In turn, Americans are facing an affordability crisis; the average premium for an employer-sponsored family health insurance policy reached $22,221 in 2021.6
In addition to the self-serving reasons for incorporating HEOR data capture and analysis in medical device clinical trials, it can also contribute to saving an ailing healthcare system for all. Consider this: an at-home FDA-cleared ECG monitor such as KardiaMobile plus a smartphone can monitor for early signs of heart failure, not only thwarting would-be heart attacks but also the high costs of emergency room visits. Further, compared to the $3,000 to $10,000 cost of testing at a medical facility, the cost of testing using a remote ECG device is only about $200.7 That reduces the cost of testing for patients, providers, and payers.
Any medical device—digital or otherwise—that supports staying at home or prevention has a dramatic impact on the financial health of the broader medical community. After all, more hospitals are trialing the hospital-at-home concept, but this is only feasible if the costs support it. Johns Hopkins reports a savings of 19% to 30% when compared to in-hospital care.8 It’s yet another critical reason to incorporate HEOR data capture into clinical trials, especially longer trials.
Joel Morse is co-founder and CEO of Curavit, a virtual contract research organization that designs and executes decentralized clinical trials. He is an experienced operational CEO who has founded, built, and sold large global businesses in healthcare and life sciences. Previously, Morse founded C3i, a business process outsourcing healthcare provider, and built it into a global leader in tech-enabled clinical trial services, with a strategic client list that included Medidata, Quintiles, and Merck. Morse has a BS in mechanical engineering from Tufts, and an MBA from Columbia. He can be reached at joel.morse@curavitclinicalresearch.com.
A digital therapeutic (DTx) is defined as “health software intended to treat or alleviate a disease, disorder, condition, or injury by generating and delivering a medical intervention that has a demonstrable positive therapeutic impact on a patient’s health.” The digital health industry has been through a series of cycles and novel DTx are starting to emerge following changes in the regulatory framework and reimbursement environment. This has reignited investor interest and the field is now ripe for partnerships with the pharma industry.
DTx have been a transformative force in healthcare, providing an alternative evidence-based intervention to drugs and medical devices in the prevention, management, and or treatment of medical disorders. During the COVID-19 pandemic, DTx took on a new lease of life. Many start-up companies used the lenient regulatory environment to pilot new digital tools in various therapeutic fields.
However, in 2023 the market leader Pear Therapeutics’ filed for bankruptcy, raising concerns over whether DTx were commercially viable. DTx companies were forced to re-evaluate their business models and many companies merged. Akili Interactive was acquired by Virtual Therapeutics for $34 million, Click Therapeutics obtained the assets of defunct Better Therapeutics and Pear Therapeutics. DarioHealth expanded its digital offerings for chronic conditions with the acquisition of Twill, Mahana Therapeutics acquired Berlin-based Cara Care, and Aptar Digital Health acquired Healint to enhance its portfolio and drive growth.
Dave Hanaman, CEO and co-founder of Curavit Clinical Research, US, notes that: “The digital landscape has experienced a fluctuating investment cycle that has risen, fallen, and then risen again. DTx, along with other digital solutions, were promising nascent industries before COVID, and post-COVID there was a bit of a fallout in the digital health market. The highs and lows have been amplified by COVID, but in the long run smart business models have emerged and the industry is back on track to deliver strong steady growth and value to payers and sponsors.”
The Digital Therapeutics Alliance (DTA) has worked tirelessly to educate stakeholders and has lobbied for changes in healthcare policy to improve the coverage and payment of DTx. In the US, the Access to Prescription Digital Therapeutics Act introduced in 2022 helped to define the reimbursement benefit categories for DTx and increased the provision for Medicare and Medicare coverage of prescription DTx (PDTs). In July 2024, the Centers for Medicare and Medicaid Services (CMS) released a new payment policy proposal to provide new codes for the use of digital tools that support the delivery of behavioural health. More recently, H.R.8166 has been introduced in the Medicare supplemental agreement to provide clarity for Medicare Advantage plans.
In Europe, France and Germany have paved the way in DTx innovation by establishing regulatory frameworks and reimbursement models, and other regions, such as Asia-Pacific (APAC), are looking to embrace and integrate DTx’ into the healthcare ecosystem.
According to Andy Molnar, CEO of the DTA organization in the US: “During the last few months, however, we have seen a lot of DTA’s hard work pay off in the form of health policy updates; CMS 2025 Proposed Physician Fee Schedule (PFS) has been released that includes three new codes to cover digital mental health treatment (DMHT) devices and this is a huge step forward. Plus, these changes are tracking internationally, with processes in Germany, France, South Korea, and Japan covering prescription DTx.”
“As the regulatory framework has evolved, the industry has been working on next-generation products,” he continued, “and we are going to see a sharp uptake in innovative products entering the market in the future.”
Recent product approvals
There are now several routes for regulatory approval of DTx based on the positioning of the product, which has de-risked the DTx development process. The FDA has established a Digital Health Advisory Committee (DHAC) to bring stakeholders together to assess digital health offerings and the DTA recently announced its plan to launch an accreditation programme to help DTx manufacturers to assess clinical efficacy and select programme(s) that are appropriate for their business models.
In the last year, several PDTs have received FDA clearance, including Click Therapeutic/Otsuka’s Rejoyn for the treatment of major depressive disorder (MDD), Freespira’s at-home treatment to reduce and stop panic attacks and post-traumatic stress disorder (PTSD), and MedRhythm ‘s MR-001:InTandem for neurorehabilitation in patients with multiple sclerosis (MS), Parkinson’s disease, and chronic stroke. In 2022, Biogen entered into a $3 million development and commercialisation agreement for the PDT to address gait deficits in MS patients.
In June 2024, Akili received FDA approval for EndeavorOTC, its over-the-counter DTx for attention deficit hyperactivity disorder (ADHD) in adults. Alkil already had FDA approval for the prescription version of the interactive video game for children with ADHD, but had struggled to make it commercially viable; the new indication will help expand its use and make it more accessible to those in need. In addition, Hinge Health expanded its DTx solutions and launched a DTx to support menopausal women who experience musculoskeletal (MSK) and pelvic health issues. In April 2024, Curio Digital Therapeutics received FDA 510(k) clearance for its postpartum depression.
Leveraging real-world evidence
DTx have become more widely accepted by the medical community and patients. Increasingly DTx companies are undertaking more in-depth studies, including randomised clinical trials (RCT) and real-world evidence (RWE) studies to support their approval and coverage. For example, in May 2024, German-based GAIA initiated an RCT involving 348 participants to determine the impact of Klariva on the Dermatology Life Quality Index, psoriasis severity, and depressive symptoms. GAIA already markets the DTx for the treatment of psoriasis in Germany, but this data will help differentiate the product and secure its continued reimbursement by payers.
According to Hanaman, “DTx companies are leveraging RWE in a couple of important ways, and this is where decentralised trials are supporting the DTx space. It is feasible to not only look at the safety and effectiveness of DTx, but to also generate RWE to understand the health economic impact of the therapy on the individual, plus the healthcare system as a whole.”
“By looking at data over time, we can see the long-term impact and support of the product’s application and commercial rationalisation,” he continued. “In addition, companion apps are evolving to support patient management, monitoring the effect of traditional therapies and lifestyles on disease symptoms and side effects across large patient populations over time.”
In oncology, DTx companies have started to leverage digital solutions in disease management. Earlier this year, Mika Health partnered with the global non-profit Cancer Support Community (CSC), and Health teamed up with Gerresheimer, to develop tailored DTx to support patients, caregivers, and healthcare professionals in cancer therapy management. In 2022, DarioHealth and Sanofi entered into a multi-year, $30m strategic agreement to help accelerate the commercial adoption and expansion of the Dario platform, which helps patients manage chronic diseases, including diabetes, hypertension, weight management, musculoskeletal, and behavioural health.
Pharma’s renewed interest in DTx
According to Molnar, now is the right time for pharma to partner with DTx companies.
“There are several routes for reimbursement of DTx based on the positioning of the product, and this is starting to de-risk various models, including pharma partnering with DTx manufacturers,” he stated. “Pharma is getting more involved in patient management of disease and the FDA has defined the Prescription Drug Use-Related Software (PDURs) pathway. This enables pharma to add value to existing pharmacologic interventions where the DTx can help to manage the disease or side effects of drugs and be used to differentiate products and bring value to the patients on a global scale.”
Several pharma DTx partnerships have been announced in recent months. In July 2024, Otsuka forged an alliance with Health Innovation Oxford & Thames Valley (Oxford HIN) to evaluate the implementation and integration of a new DTx, CARE for MDD. In March 2024, Teva UK announced a strategic partnership with Closed Loop Medicine to use its proprietary software as a medical device (SaMD) as a digital companion to pharmaceuticals to advance the development of personalised medicines. And, in January 2024, Orion Corporation and Newel Health entered into a licensing agreement for Virtual Reality DTx Rohkea (ODD-403) in chronic pain.
DTx are here to stay…
Healthcare systems around the world face increasing pressure to provide improved population health outcomes at lower costs, and technology including DTx will play an increasingly important role in care delivery.
“There are gaps in the healthcare system that can only be solved with DTx,” noted Molnar. “We have an ageing population and there are not enough doctors to take care of people at home 24/7, but there are DTx that can do that.”
Hanaman agrees.
“The future of US healthcare is the future of digital,” he said. “All types of digital medicine, including DTx as standalone solutions and in combination with traditional therapies, will be fully incorporated into the healthcare system, in the same way the internet has been incorporated into businesses.”
“DTx will be supportive in driving healthcare outcomes for our lifetime,” Hanaman concluded.
Decentralized clinical trials (DCTs) are shapeshifting.
Originally piloted 15 years ago and more recently catalyzed by the COVID-19 pandemic, DCTs took center stage in 2020 and 2021—mostly out of necessity, but with great promise for their potential to dramatically improve patient access, enrollment, trial speed, data quality, and population representation. Now, in the third quarter of 2024, the market landscape looks less rosy than the earliest depictions.
While the value of the global DCT market is projected to increase over the next six years from $8.5 billion in 2023 to $13.3 billion by 2030 (growing at a compound annual growth rate of 6.6% in the forecast period), these projections are lower than they were in 2022. Other financial indicators suggest that the market remains volatile. According to LinkedIn employee data, the number of employees in companies most aligned with providing DCT software has declined over 20% from their highs.1 In DT Consulting’s new report, “State of Digital in Clinical Operations 2023,” two-thirds (69%) of respondents said they expect their digital budgets to stay flat or decrease.2
Even so, in the uber conservative clinical research industry where people’s lives are at stake, the fact that DCT excitement has tempered from a rolling boil to a gentle simmer is hardly surprising. Even in less risk-averse industries, adoption of disruptive technologies tends to follow a natural slackening, as noted by Gartner’s Hype Cycle.3 Have we hit the “peak of inflated expectations” with DCTs or the feared “trough of disillusionment”?
One of the issues is that sites and sponsors are facing challenges with adoption of decentralized elements. An Association of Clinical Research Professionals survey reveals that sites lack the training and budget to implement DCTs.4 Additionally, the top-cited reason sites declined participation in decentralized trials in another survey was hesitancy to adopt these methods without a sufficient budget to cover additional training or the integration of new technologies.5
Decentralized methodologies remain a stable feature of trial activity, albeit at a lower level after the COVID peak in 2020, and the negative news does not diminish the positives of DCTs. The question remains: Is this study model a bust or a breakthrough? Time will tell, but certainly DCTs are changing shape.
Ahead, five industry leaders, each with deep-domain experience designing, implementing, and measuring DCTs, provide their perspectives on how these types of studies are evolving and their impact on an ever-changing research industry.
1. Ken Getz, MBA, Tufts CSDD Executive Director
The Tufts Center for the Study of Drug Development (CSDD) in collaboration with the Partnership for Advancing Clinical Trials (PACT) consortium recently revealed compelling results from a new study on 60 clinical trials that deployed decentralized solutions.6 Funded in its first year by the Reagan-Udall Foundation and Medable, the consortium is committed to collecting and analyzing evidence on DCT experience and its impact on trial performance.
PACT member companies indicated that they anticipate one-third of all protocol procedures, and half of all study visits, could be performed remotely. And companies use, on average, four distinct DCT solutions per clinical trial, most often in support of study visit activity.
In this initial dataset, wide variation was observed in the ways that companies deployed DCT solutions. Select outcome measures—such as screen failure rates, participant completion, and dropout rates—were similar to industry benchmarks, although many of the clinical trials using decentralized elements had not yet completed enrollment. On the other hand, actual timelines for clinical trials supported by decentralized solutions were more likely to beat planned timelines from first site activated to first patient enrolled, and from first patient to last patient enrolled. The results also showed that clinical trials using certain DCT solutions were associated with more diverse patient demographic representation.
Next, Tufts CSDD and the PACT membership will work to increase the size of the analysis dataset and generate more granular insights in year two to inform DCT adoption and optimize use by disease condition, patient preference, and other factors.
Trials using technology or local facilities have been around in one way or another for decades.The use of technology matured in the mid-2010s when the nomenclature coalesced around mobile, digital, and virtual clinical trials and exploded during the pandemic as DCTs. We had hoped that the pandemic would have allowed DCTs to fly over the trough of disillusionment but, as the Gartner Hype Cycle predicts, we find ourselves following the curve.
The nomenclature used for decentralized trials is still evolving, and we will likely abandon the DCT reference altogether someday. Instead, we will simply deploy various decentralized elements in trials in a fit-for-purpose way based on where they are best suited based on evidence (i.e., such as the PACT Consortium’s recent report around DCT impact on diversity). In the same way we no longer specify whether we have a “paper” boarding pass or a “digital” boarding pass—just a boarding pass—we will just say we are running a clinical trial.
Adoption of novel clinical trial methodologies is tricky. A 2023 Tufts CSDD Impact Report indicated that it typically takes six years for a company to adopt an innovation and 20 years for widespread adoption.7 Yet, digital endpoint use has doubled every three years since 2015, so there are signs of growth. With harmonized regulatory guidance, adapted workflows for sponsors and sites, an optimized site experience, better platform technology, and evidence of value, the industry will rapidly embrace decentralized trials again. Sponsors will surgically apply the right elements to accelerate reliable evidence generation while keeping participants safe.
3. Daniel Eisenman, PhD, Advarra Executive Director of Biosafety Services
As DCTs started gaining momentum during the pandemic, researchers were quick to put guardrails around their use, saying that highly complex or logistically unique therapies would not be candidates for full decentralization.8 Oncology, for example, was too risky for a fully digital-based trial. However, that belief has changed with the availability of new treatments such as targeted medications, drugs that can be administered orally or subcutaneously, and the ability to provide home infusions. And, with the emergence of hybrid trials that blend digital tools with some in-person visits, there is now even more flexibility with this model. In fact, today, oncology ranks in the top five therapeutic areas leveraging the decentralized model for trials.9
The same benefits that DCTs bring to other therapeutic areas apply to cell and gene therapies (CGTs), especially those intended to treat rare disease patients. It is difficult to recruit patients with a specific rare disease in numbers large enough to produce meaningful results in a clinical trial—especially if scattered over a wide geographical area. DCTs allow for remote tasks and data collection, which reduces the responsibilities and limitations of local sites, allowing for a larger trial network, which can serve a greater number of participants. Yet, the same lingering doubts around the viability of a DCT in oncology a few years ago have blossomed forCGT trials.
Traditionally, CGTs come with complicated logistical requirements—temperature-controlled shipping, safe storage, unique administration of the drug—that were not conducive to a DCT. However, CGTs are evolving just as DCTs. For instance, some investigational CGTs fit the criteria for DCTs while others do not.
One example of a CGT that has less rigid handling requirements and would be a good candidate for a hybrid DCT is freeze-dried bacteria (a live culture genetically engineered) that comes in a packet that patients simply mix with water. Other examples are CGTs that come in the form of topical ointments or nebulizers to be inhaled.
The bottom line is that we cannot rule out DCTs for the rapidly advancing area of CGTs. DCTs could prove to be the key to furthering the development of this incredible science and finding treatments for diseases that have been untreatable. We cannot dismiss DCTs outright—rather, adopt modern trial designs carefully and fit-for-purpose.
As an industry, let’s start each trial asking if it is well-suited to be a hybrid DCT based on all underlying factors, from patient safety to costs and everything in between. For CGT decentralized trials, especially, we need to identify the “Goldilocks zone”—not too much, not too little—just right for the science.
4. Troy Astorino, PicnicHealth Co-founder and Chief Technology Officer
The premise behind DCTs is sound: reduce dependency on overburdened sites and improve patient participation and diversity. However, COVID drove wide-scale DCT adoption before the technology was ready, resulting in broad industry disillusionment. Researchers using DCTs faced major challenges due to technology immaturity, lack of hybrid-native solutions, and narrow data capture capabilities.
Early DCT systems struggled to power smooth, integrated end-to-end trials. This led to friction for all stakeholders and made implementations feel “heavy” because extensive workarounds were needed. Many trials require a mix of site-based and remote components, especially for complex treatments, and initial approaches didn’t effectively accommodate this reality.
Replicating the breadth of traditional site-based data capture, particularly for endpoints sourced from electronic health record (EHR) data, proved challenging for DCT designs.
In response, many DCT providers have pivoted to offering point solutions, such as eCOA or eConsent, which can be more easily integrated into trial designs. While practical, this approach doesn’t fully realize the transformative potential of DCTs. It is important to first identify where virtual and hybrid approaches can truly excel. Observational research has proven to be a successful starting point.
Traditionally, observational studies have been awkwardly forced into site-centric models designed for interventional trials, leading to inefficiencies, high dropout rates, and potential data loss. Two capabilities are crucial to unlock decentralization in observational research. First, comprehensive EHR collection that integrates patient records across all providers to capture a more complete picture of patient health. Second, remote patient engagement to facilitate various forms of active data collection from patients where they are comfortable to improve participation and data quality.
Combining these capabilities creates a solid foundation for virtual and hybrid observational studies. They address the data capture challenges of earlier DCT models while maintaining the benefits of reduced clinical site burden and improved patient accessibility.
Additionally, a unified trial platform simplifies deployment of advanced technologies, including artificial intelligence (AI), across all components of a trial. AI is advancing rapidly to streamline processes, enhance data quality, and generate deeper insights. Limiting technology innovation to DCT components fails to leverage the full potential that modern technology platforms can deliver.
While the early hype for DCTs has subsided, the fundamental opportunity remains. As the industry refines its approach, we can expect to see more efficient, effective, and patient-centric clinical trials, particularly by focusing on strategic applications such as observational research first. This evolution will likely accelerate therapeutic development and, ultimately, improve patient outcomes.
5. Joel Morse, Curavit Clinical Research Co-founder/CEO
The promise of DCT 1.0 has not materialized for three reasons. First, clinical research is a risk-averse industry that typically applies changes thoughtfully, but the pandemic necessitated hasty adoption of DCT technologies.
Rushed implementations sometimes resulted in missteps, so the full potential of DCTs didn’t emerge as fast as expected, causing the industry to rethink their strategies, slow down, and become skeptical.
Second, inflated expectations of DCTs spread like wildfire. These unrealistic expectations became the new measuring stick for DCT success or failure, but it was a manufactured target, and sponsors grew wearier as the goalposts changed. Companies singing the praises of DCT software platforms were now changing their tune. Again, this fueled (undue) skepticism.
Third, the industry focused too much on the software and less on a comprehensive set of data and the overall clinical trial execution requirements. We oversimplified what it would mean to run a decentralized trial by thinking that great software would drive widespread adoption, but technology cannot single-handedly transform a model that has largely been handled the same way for decades.
We now have a deeper understanding and are learning from early mistakes. To fully realize the potential of DCTs, we must realign processes to digital workflows. This includes supporting the collection of comprehensive data sets, optimizing recruitment of the target patient populations, and leveraging both virtual and physical sites.
This holistic approach to trial design will drive the next evolution of clinical trials. DCT 3.0, focused on digital-first principles, is poised to meet the original expectations. DCT 3.0 will be grounded in purpose-built virtual sites, which will serve as the central hub for trial activities and clinical data, coordinating the entire trial.
The most important perspective: The patient
Rita Naman, co-founder of the Mighty Milo Foundation,10 is hopeful that digital technologies and decentralized methodologies will continue to mature and expand. Naman is the mother to 5-year-old Milo, who has SPAX5, an ultra-rare, serious, and inherited neurodegenerative disease that affects children early in life and is characterized by problems with balance, motor coordination, spasticity, peripheral neuropathy, and more. Milo is one of 12 documented cases. There is no cure, so access to investigational therapies is Milo’s best chance for help.
“The value of DCTs, especially for rare disease research participation, cannot be understated,” says Naman. “My son has significant caregiving needs that make it difficult, if not impossible, for him to participate in far-away trials. I pray that this industry will continue to be our beacon of hope and that no one gives up on modern alternatives for research such as DCTs just because technology investment has slowed. Digital tools can open new doors to patients like my son, who face endless, heartbreaking challenges.”
A lot has happened since the onset and passing of the COVID-19 vaccine national public health emergency. Decentralized trials were a hot item, and Curavit was one of a few startup ventures helping sponsors to decentralize their research, bringing studies to the community and even the home. But a lot has changed since the passing of the pandemic as hybrid studies remain the norm—that is, studies that include traditional elements plus digital tools for decentralized engagement. Enter Curavit, a serious decentralized contract research organization (CRO) led by pedigreed operators.
Both CEO Joel Morse and President and Chief Commercial Officer Dave Hanaman were behind the clinical trials technology support and services company C3i Healthcare Connections, a Division of Telerx. The pair and colleagues scaled up a global high-quality services organization and understand the challenges of execution in Food and Drug Administration regulated environments.
Pamela Tenaerts, MD, MBA, chief scientific officer, Medable; Luke Gelinas, PhD, senior chair director, Advarra; and Pam Diamond, MD, chief medical officer & co-founder, Curavit highlight the potential impact FDA’s Diversity Action Plan guidance will have on industry.
Tenaerts: I think it’ll help the industry get more data, actionable data on a diverse population—there’s different ways to do that. You can change your inclusion/exclusion criteria. You definitely work with the communities. It’s also becoming clear that decentralization could be part of the how you get there. You have to have your goals reflect the population and then you have to have the rationale of why you picked those percentages or those things, and then one of the things that’s emerging is that decentralization could be one of those things. We had some recent data come out from the PACT (Partnership for Advancing Clinical Trials) consortium that showed that using decentralized elements, there’s an emerging trend of more diversity, with less white people enrolled and more Asian people enrolled, so I think we want to get more data on that, but it’s important that the industry is moving in that direction, and that we’re all doing the right thing.
Gelinas: It’s going to force industry sponsors to think really carefully about the types of patients they’re trying to reach with their drugs, about what they think representative clinical trial sample looks like. I think it’s going to force us a lot more critically and deeper than we had before about what diversity means and what aspects of it are important in terms of sex, ethnicity, race, gender—those are the ones that FDA guidance is focused on. I think it’s going to be positive in the sense that it’s going to force the industry to step back and say—for each different drug that are assessing or device—what is the patient population that we’re hoping to reach with this drug or device look like in the real world? That’s really what we should be using to draft our diversity plans for clinical trials. We should be trying to capture the patient groups in terms of demographics that you’re actually going to serve with the product, the people who are going to take the drug or device, should it become available on the market. It will be good in that respect, and helping industry to think hard about those things. Again, I think it’s always good to have a plan. This is the first step in actually increasing diversity, but I think there’s more work to do beyond the plan, but again, good first step.
Diamond: I could see a short-term consequence, that early on, it might actually increase the expense that sponsors will have in conducting clinical trials. It will be more expensive to recruit a more diverse participant population, and to retain those participants, but I’m very hopeful that in the long run, sponsors will be able to save both time and money—financial resources—in the long run, because we’ve all seen trials that were not very representative, and a lot of money and time were spent on that trial, and it turned out that—say if it was a drug that was under testing—the drug wasn’t really effective in populations that weren’t part of the clinical trial. I’ve seen numbers like one and a half billion, or even in excess of one and a half billion, to bring a drug to market, so if you spend all that money and then when it goes to market, it really isn’t helping the patients that have that condition and that need that medication, it’s a lot of time and money wasted. Again, I see short run, we might have to spend a little bit more money, but in the long run, I think we’re going to see more efficiency and savings. The other thing I could see happening if we’re all really good at following the FDA guidelines is that more trial activities will be done virtually in order to enroll and retain more diverse participants. We just have so many individuals that don’t live close to academic research sites, or even physical clinical research sites, and it would be really good if we could bring more of those participants into clinical trials. Hopefully, and it’s something that our company, Curavit focuses on, is doing as much of the trial virtually as possible, so that we can engage diverse participants and keep them engaged throughout their trial.
Pharma Pulse 7/3/24: Reactions to New FDA Diversity Action Plan Guidance, Walgreens Strengthens Support for Children and Adults Living with Diabetes & more
Pamela Tenaerts, MD, MBA, chief scientific officer, Medable; Luke Gelinas, PhD, senior chair director, Advarra; and Pam Diamond, MD, chief medical officer & co-founder, Curavit share their initial thoughts on the announcement of FDA’s Diversity Action Plan guidance.
Scarcity of data and siloed data sources lead to gaps in information that create challenges in study design. Additionally, the increase in trial complexity, which has seen a 600% increase in collected data points, contributes to a negative impact on a variety of trial performance outcomes. Evidence-based insights help study teams iterate upon ideas that can lead to lean study designs, resulting in reduced data points, decreased costs, and less deviations.
This webinar uncovers how technology and analytics can be applied to address key areas during study design/synopsis development. Learn how design analytics can help sponsors make early, in-flight design decisions prior to protocol authoring, such as selecting best endpoints, determining which eligibility criteria will improve probability of success, and identifying key regulatory design considerations.
The retail pharmacy chain will highlight a variety of offerings and healthcare solutions for managing diabetes at Friends for Life Conference hosted by Children with Diabetes.
Understanding the Impact of the Veradigm® Network on Value-Based Healthcare Delivery
Learn more in this article about how Veradigm®’s comprehensive network and data capabilities support biopharma in achieving patient-centered, cost-effective care.
Read the Article: https://ow.ly/MQxL50SkmW1
Have news you want us to share in Pharma Pulse? Reach out to Social Media Editor Miranda Schmalfuhs
On May 16, 2024, Applied Clinical Trials held a roundtable event focused on the current state of sustainability in clinical research. A number of viewpoints were represented, including from contract research organizations (CROs), sponsors, and laboratories. Experts discussed a variety of topics, such as the carbon footprint of research, the use of technology, reaching underrepresented populations, and the clinical supply chain.
ACT: What is the current state of sustainability in clinical research? What are currently our greatest challenges?
Bill Sterling, Senior Director of Environmental, Health and Safety, Q2 Solutions:
Bill Sterling
Bill Sterling
I think there’s growing enthusiasm. There’s certainly a lot of enthusiasm at Q2 for sustainability initiatives. There’s a sense of pride as employees start to see that this is a high priority and an uptake at the highest levels. That’s been exciting to see. I think things are really growing and expanding in this area. In general, laboratories can be particularly challenging in terms of finding ways to improve sustainability given labs require energy-intensive equipment like ultra-low temperature freezers and single-use plastics for safe sample collections.
Ingrid Oakley-Girvan, PhD
Ingrid Oakley-Girvan, PhD, MPH, Senior VP of Research and Strategy, Medable: I’m really pleased by the number of our customers that are reaching out to ask us, “Do we have a sustainability plan? Have we started this process?” It’s really heartening to see that there is concern about that and assessing where the gaps are and areas with the greatest potential impact. If you’re just expending a little bit of energy in one place and you put all your eggs in that basket to try to solve that problem—water, or greenhouse gases, etc…from the sustainability metrics—then you can’t get that far. But if you know where there’s a big chunk, that’s the piece that you can focus on, and I think that’s part of why they’re asking us.
Cedric Burg
Cedric Burg, Chief Operating Officer, Innovaderm: I would agree. I would add, I think we’re not one of the big polluters, right? We’re not the mining industry or the oil and gas industry; but what our biggest impact is, apart from the facilities that you both were mentioning as well, I think is the travel. We do a lot of travel to run clinical trials. We organize those large investigative meetings, people flying in from all over the country or all over the world. And of course we’ve got CRAs (clinical research associates) going to sites quite a bit, and, not to forget, we’ve got patients going to sites as well.
I think our biggest challenge is that because we can do a lot of things, we’re still going to need to do quite a bit of travel, and the more trials we’ll do, the more travel. Unless we see a complete decarbonization of travel, we will still have that impact and have to find other ways to mitigate it.
Bryan Spielman
Bryan Spielman, Chief Growth Officer, Advarra: It’s hard as a software company when you respond to surveys from pharma companies—we are not a manufacturer, we are not a lab, we don’t do that sort of stuff. But what we do have is a great deal of data that helps you determine what is the optimal site to perform a clinical trial, who are your best patients, what capabilities do those sites have, so that instead of going to 10 different places to hit all the different experiments that [patients] need to have done, [you discover] the one site that has all of them—so let’s direct trial activity to those places. I think using data, using analytics to help improve the operational efficiency of a trial is much better than putting my laptop on low power mode. It’s going to have a lot more of an impact, frankly. And those are some of the ways that we’re thinking about it.
ACT: With the complexity of rare diseases trials, sustainable practices might be less of a priority. Should companies face up to their environmental impact at the risk of thousands of rare disease patients potentially missing out on a therapy? What’s the trade-off? Is there a way to balance the two?
Dave Hanaman
Dave Hanaman, President, Co-founder, and Chief Commercial Officer, Curavit Clinical Research: The direct answer in my view is no. The research, by definition, is the priority. Priority means “first”—there’s only one first we’re about: research. We can affect research. We are not going to invent the technologies that are going to save the planet. Now, that said, we can be efficient, we can be effective, we can choose sites that are efficient, and do a good job. Those are the things we can do. There is only one priority and that’s the research—and that’s for the patients.
We can and should do these other things, but not in any way, shape, or form that impacts the ultimate research.
Oakley-Girvan: I think there’s also this assumption that if a patient with a rare disease enrolls in a clinical trial, somehow that has a greater carbon footprint than what they would do otherwise if the trial wasn’t available. I’m not sure that actually is an accurate assumption because [patients] could be traveling hither and thither looking for a cure. They could actually have a greater travel carbon footprint, for example, than if they just go to a specific trial site that might be in the same country versus multiple countries away.
Sterling: Yes, there is a way to balance the two in terms of trade-offs. I think there’s impact in terms of human quality of life and longevity with regards to rare disease, but there’s also an impact to using dirty energy to achieve it. The emissions of greenhouse gas and other pollutants into the air have an enormous impact on human health. So it’s absolutely both. First and foremost, the reason to advance these ambitions is it’s the right thing to do. We all know that—we’re all here because we care about the environment.
There are certainly increasing regulations, and meeting those regulations is something that needs to be done. But, also, there are often cost savings that can be uncovered; often, it supports business growth. Our shareholders and our clients are pushing this program as well. It’s about aligning to a competitive market and, in addition, attracting and retaining good talent. I mentioned that a number of our employees get really excited when they’re involved in the laboratory green teams or when they see leadership championing sustainability ambition. So it has to be both.
Julia Sundari
Julia Sundari, Senior Director of Clinical Design and Analytics, IQVIA: I don’t think it always has to be a disadvantage to our businesses when we focus on sustainability. Because if you can be out on the forefront of this, then your sponsors are going to want to turn toward you if your carbon footprint is lower and if you can offer a clinical trial with a smaller carbon footprint and you have solutions to some of these things. [After all,] they’re looking to do that themselves.
So, from the sponsor down—everybody as a human being on the planet earth—we all really serve the end game of accomplishing this together, whether it’s at work or whether it’s personally in our lives.
ACT: One of the longest-standing challenges in clinical trials over the years has been patient participation, especially within underrepresented populations. How can we address this to make trials more sustainable?
Hanaman: Greater diversity and better efficiencies are important pieces in our experience. [But] the dominant opportunity here is in speed. The faster we do something, the less energy we’re using in conducting it. And then, secondly, the adherence. The more patients we can keep in a trial, the better the adherence, the better the data, potentially, the shorter the trial, etc.
Sundari: We want to make sure that we don’t forget the carbon impact. So while, absolutely, DCTs (decentralized clinical trials) can impact carbon from a positive effect, at times it’s neutral. If we’re just replacing an on-site visit with a home health nurse physically still traveling to the patient, then it may net the same amount of carbon being used. I think it’s certainly about the design, it’s about looking at how many of these things can we make virtual, how much of the data can actually be wearable, or other ways where it’s electronic data capture directly from the patient. And then, of course, the more we centralize, the more carbon neutral we become, because we hopefully don’t need to physically go to places to see that data and monitor that data.
Spielman: I think along those lines, injecting technology into sites that have been less research-intensive is also important.
We are partnered with Novartis on its Beacon of Hope initiative, which is about creating centers of excellence at historical black colleges and university medical centers. Why is that good for sustainability? One, we talked about the idea of sustainability—about bringing underserved populations into the process. Two, it’s actually bringing the clinical trial closer to those underserved populations that live in those communities where those medical centers are educating doctors to be able to serve those communities. And I think it’s creating the “clinical research as a care option,” which is also a sustainability benefit.
ACT:Technology use is increasing rapidly in clinical trials, especially with the boom of AI and wealth of available data. How is it being used to make trials more sustainable?
Sundari: The way I see AI directly impacting the clinical trial space is around leveraging that information on our data. So targeting analytics and machine learning so that we can mine that incoming data remotely—physically have boots on the ground at the site but internally consuming that data and understanding where the risks are and correcting them more quickly, even in the middle of a trial. And being more environmentally sensitive to where we actually do need to send those monitors to the site.
Spielman: I would say AI/machine learning has so many different applications across each of the areas, and anytime you’re driving efficiency, you’re probably doing something that’s more sustainable. With protocol design, for example, it’s making sure you get it right the first time so you can minimize the number of amendments and modifications that need to be made in the trial to the extent it’s feasible. There’s also quality monitoring, there’s the ability to ingest large amounts of data and determine which sites are our potentially problem sites, and then you deploy your CRAs to those sites as opposed to every single site, which is pretty inefficient.
There’s all sorts of applications, but I think the easiest one is trying to reduce the amount of bodies that you have to send out to various locations.
Burg: I want to raise the other side of the issue. I think there’s also a big risk to using AI in our work, which can create a lot of work that is not necessarily needed. When I started, we had monitoring plans that were half-a-page or a page-long. Now we have 50 page-long, 80-page long monitoring plans. Because we can probably easily do it with AI, I’m afraid we’re going to turn out 180-page or 200-page documents, perfectly written and very well organized without all those typos, but that are really not going to help the monitor. That’s my worry. We also have to be careful about all the new technology because sometimes there’s a lot of hype around it.
ACT: What are some roadblocks we are currently facing in the clinical supply chain? How can they be addressed?
Sterling: It’s really a challenge in terms of conserving energy in a laboratory. You’ve got a very large need for energy with regards to HVAC systems, fume hoods, clean air, single-use plastics, and so forth. One of the things that has been extremely helpful for us is partnering with a group called My Green Lab. It’s a nonprofit organization that essentially provides a scored self-assessment survey training across 14 different topics that map onto laboratories. Topics like cold storage, green chemistry, fume hood use, and plug load for equipment.
Starting in 2022, we launched into the My Green Lab certification process to assess our baseline practices. It created a lot of enthusiasm, a roadmap, and a structure for people to latch onto to learn about and engage various sustainability programs and projects. The most important thing is we’ve delivered some real carbon reductions and provided value for our clients. It means something to them for us to be able to say, “These sites are platinum, these sites are green-certified as the highest you can get—gold and bronze and so forth.” It gives sites a tangible roadmap and ambition to move upwards on the podium.
Oakley-Girvan: That sounds like a great program. I know we’ve been working with some of our customers that want us to do what’s called a RAG, a red-amber-green assessment, every 60 days. This includes science-based target initiatives. If we’re sending out sensors, we’re thinking about the packaging, all the energy that goes into making those, how can our sensor vendors be more efficient? That’s a big space.
Hanaman: In terms of sustainability goals, I find it almost funny the paradox, in my experience, of DCTs and remote data capture. The paradox is that there’s a lot of “stuff” now that you’ve got to get out to the patients. It used to be all the “stuff” was at the sites and the patients just had to get there. I think this logistics question is a really important one because the more we take advantage of these digital processes and technologies, the more we as CROs, sponsors, and companies take on the challenge of getting this stuff out to the participants in the trial.
There’s a couple of different ways to think about that. One is simply that policy and regulation can drive this a little bit. The other is thinking about medical grade products and the cost and the energy that it takes to build them. What is it we’re trying to collect from that patient? Do we need to spend ‘X’ and do it using an Apple Watch or do we have to spend ‘10X’ for some medical grade component that has a much heavier energy footprint and is thrown out after the trial?
There are so many products out there that don’t have to be reinvented for clinical trials, don’t have to be reinvented for care—but can simply be repurposed through algorithms. So just creatively thinking about simple ways to get simple products out into people’s hands.
ACT:What does having more sustainability in clinical trials look like from your perspective in five years? What do you hope the industry can accomplish by then?
Sundari: I feel like we’re on sort of a wave where more and more companies are getting to the point where they’re willing to commit to their goals—their science-based target goals—and having those approved. I would say that would be the first step for wherever you sit in the business—to make sure that your company, your corporation, your part of this industry is focused on it.
I think for clinical trials at large, we touched on many of the things that I would say are probably the handholds or footholds. It’s digitizing for sure. It’s making sure that we’re using technology to our best as far as the end-to-end supply chain; making sure that we’re designing protocols as intelligently as possible; and that we aren’t incurring additional manufacturing, shipping, and travel wherever possible. However, how we can do those things most intelligently across the board is really the goal.
Sterling: And to build on that, Julia, you mentioned SBTI—the science-based target initiatives. I think transition to renewables at a number of our sites is important, either through purchase agreements or installations and packaging in kits that go out to patients. Reworking those so that they’re sustainable. I also spend a lot of time thinking about culture because I’m in environmental health and safety and sustainability; both of those things really depend on employees being energized and engaged and having a sense of ownership.
I see that happening already, but in five years, my hope is that it’s even stronger and it’s something that we see around the world. I think we have an opportunity as the younger population is coming into our workforce to take advantage of the fact that they really care about this.
Hanaman: We’ve talked about a lot of technologies today, such as AI, that are creeping in upstream from us and already being adopted. So I think at a very simple level, those things will be flowing through to us and will be more sustainable as a result.
But I’m going to pick up on Bill, who mentioned the word culture. To me, the big driver here is that in five years, I actually think our industry is going to look a lot different, and I think it’s going to be because of, not the intersection, but maybe the collision of tech and health. We’re a small segment of the healthcare industry. I think the industry is going to be radically disrupted in the next three to five years by these technologies, but more importantly, by the culture and by the people that we’re going to have around us and part of us in designing these things.
I think it comes down to folks like us on this call designing these trials from first principles—not designing them the way we’ve always done and then shoehorning technology into them, but designing them from first principles with a knowledge of what actually can be done.
I think that in the next three to five years, we’ll see a massive shift in that mentality.
Spielman: I think more excitement around this as a sustainable industry is actually a good marketing position to have. Again, you want to attract younger people to clinical research, and they are attracted to sites that are greener and attracted to what’s viewed as a more sustainable process. I think that will help.
Pam Diamond spent almost three decades practicing medicine and looking at problems in the clinical research arena before changing tack so she could make a bigger impact.
Could you elaborate on some of the most prominent trends shaping the landscape of clinical trials in the Asia-Pacific region?
At the geopolitical level, the rivalry and deteriorating relationship between the United States (along with its allies and partners) and China (the second largest pharmaceutical market in Asia) will continue to impact business between the two nations.
Japan remains the largest pharmaceutical market in Asia, and its improving economy and aging population will drive clinical trials for the foreseeable future. Japan also leads the region in innovation around digital health. In fact, Japan’s digital health market is expected to show a compound annual growth rate (CAGR) of 7.29% from 2024 to 2028 versus 7.48% over the same period in the U.S. It’s expected to reach $6.15 billion this year versus China, which is expected to hit about $54 million. The island nation’s leadership in digital health reflects the country’s unique blend of technological innovation, aging population, and proactive approach to healthcare challenges.
South Korea is another key player in the APAC region in biotech and digital health, and sits third in size behind Japan and China.
How do you foresee the evolving regulatory landscape in key Asia-Pacific countries impacting the conduct and efficiency of clinical trials for pharmaceutical and biotech companies operating in the region?
Australia remains a leader in clinical trials due to its world-class researchers, efficient approval process, and government support, especially in the form of tax breaks.
The Japanese government has been moving swiftly to upgrade its healthcare system with digital therapeutics and implementing forward-thinking policies and initiatives since revising its Pharmaceutical Act in 2014. The government has launched numerous initiatives over the years to promote the adoption of electronic health records (EHRs), telemedicine, and other digital health tools.
Japan’s success in digital health is also attributed to the collaborative efforts between the government, private sector, and academic institutions. This collaboration has facilitated the integration of digital health technologies into the healthcare system, ensuring that innovations are effectively translated into clinical practice. Public-private partnerships are instrumental in driving the development and adoption of digital health solutions to improve healthcare – and an area where the US is still developing.
For example, CureApp, a startup company pioneering digital therapeutics in Japan, received Japan’s first regulatory approval in 2020 for its “CureApp SC” nicotine addiction treatment app, followed by the world’s first regulatory approval for hypertension in 2022 for its high-blood-pressure-management application. These efforts are supported by policies aimed at creating a favorable regulatory environment for digital health innovation, including streamlining the approval process for digital health solutions and providing financial incentives for their adoption.
How do you see the adoption of digital health technologies influencing the future of clinical trials in the region?
The US digital health landscape experienced a major blow with the collapse of leader Pear Therapeutics in April 2023. Prior, many startup digital therapeutics and digital health companies looked at Pear as a bellwether for this fledgling industry so confidence was low. The challenges were largely financially driven by a lack of insurance coverage for these new, unproven therapies. Other companies like Akili Therapeutics took a different approach and started selling straight to consumers without a doctor’s note.
In contrast, many APAC countries can move quicker than the US when it comes to reimbursement. Clinical trials must be done on the Japanese population for market authorization in Japan, so we are seeing large growth in Japanese companies that are focused solely on the Japanese market. And you can see this through more local associations like JaDHA (the Japanese digital health association). Japanese companies have big international footprints as well, so this will certainly influence global markets.
We are also seeing a renewed interest in large pharmaceutical companies globally that are increasing their investments in startup digital health firms and offerings. One example is Sumitomo Pharma who is collaborating with the U.S.-based BehaVR to develop three virtual reality digital therapeutics addressing social anxiety disorder, generalized anxiety disorder, and major depressive disorder.
Most recently, too, Otsuka announced Food and Drug Administration (FDA) approval of its digital treatment for major depressive disorder depression. Called Rejoyn, the smartphone-based treatment was developed with US-based digital therapeutics company Click Therapeutics, and it is intended for use by prescription alongside antidepressants and cognitive-behavioral therapy. Otsuka is the first drug company to receive FDA clearance for a digital treatment for a mental health condition.
Factors that contribute to Japan’s prominent position in the rapidly evolving field of digital therapeutics and why it matters to the global life sciences industry.
Dave Hanaman, President, Chief Commercial Officer, Co-Founder, Curavit Clinical Research.
Japan’s digital health market is expected to show a compound annual growth rate (CAGR) of 7.29% from 2024 to 2028 versus 7.48% over the same period in the United States. Japan is catching some ground and it’s easy to see why. The island nation’s leadership in digital health reflects the country’s unique blend of technological innovation, aging population, and proactive approach to healthcare challenges.
“Japanese-based pharmaceutical companies have been interested in digital therapeutics (DTx) for years,” explained Andy Molnar, CEO of Digital Therapeutics Alliance (DTA). “Shionogi formed a partnership with Akili in 2019, Sumitomo Pharma partnered with Realized Care (BehaVR, at the time) in 2021, and late last year, Daiichi Sankyo announced they plan to review as many opportunities in the DTx space as possible. What we are seeing now is the result of years of interest in this space.”
Just ahead of International Clinical Trials Day on May 20, let’s dive in to understand the factors that contribute to Japan’s prominent position in this rapidly evolving field—and why it matters to the global life sciences industry.
A Flair for Technological Innovation
Japan is renowned for its technological prowess, with a long history of driving advancements in electronics, robotics, and computing. This technological foundation has naturally extended into the healthcare sector, where Japan has redirected its technology ingenuity to develop cutting-edge digital health solutions. In fact, the digital health market in Japan is expected to tower over China, reaching US $6.15 billion this year versus about $54 million in China.
From advanced wearables that monitor vital signs to sophisticated telemedicine platforms enabling remote consultations, Japan’s technological innovation underpins its leadership in digital health. For example, Takeda developed a digital therapeutic app to help monitor Parkinson disease.
Patients with this disease experience tremors and other symptoms that fluctuate in severity throughout the day and can be challenging to describe. Continuous monitoring helps physicians develop effective treatment plans, but medical-grade monitoring devices are heavy and difficult for patients to wear 24/7.
Through a partnership with Kanagawa Prefecture south of Tokyo, Takeda created an integrated care solution called “Care for One.”The solution measures Parkinson disease symptoms via an app, using a program that Apple Watch built to capture movement disorders. Patients can enter additional medical information into the iPhone app and send comprehensive data directly to their doctor’s computer.
In another example, Sumitomo Pharma iscollaboratingwith US-based BehaVR to develop three virtual reality digital therapeutics addressing social anxiety disorder, generalized anxiety disorder, and major depressive disorder. The country’s commitment to research and development, coupled with a robust ecosystem supporting innovation, has facilitated the emergence of such innovations aimed at improving healthcare delivery and patient outcomes.
Most recently, too, Japan-based Otsuka announced FDA approval of its digital treatment for major depression. Called Rejoyn, the smartphone-based treatment was developed with digital therapeutics company Click Therapeutics, and it’s intended for use by prescription, alongside antidepressants and cognitive-behavioral therapy. Otsuka is the first drug company to receive FDA clearance for a digital treatment for a mental health condition.
A Growing Elderly Population
One of the most pressing challenges facing Japan is its rapidly aging population. For the first time in the island nation’s history, more than one in 10 people are now 80 years of age or older, roughly 29% are 65 years of age or older, and by 2040, that percentage will skyrocket to 35%—including more than 300,000 centenarians.
Japan’s swelling elderly population creates unique healthcare challenges, including increased demand for long-term care and chronic disease management. Digital health technologies offer a solution to these challenges by enabling more efficient healthcare delivery, enhancing access to care for the elderly, and facilitating better management of chronic conditions.
DTx products, such as AI-powered diagnostic systems and mobile health applications, play a critical role in providing personalized and accessible care to Japan’s aging population. For example, Japanese startup Iris built an AI-powered device called nodoca to diagnose influenza within seconds without painful nasopharyngeal tests or long waits in the office.
The company trained its AI model with more than 500,000 throat images, supplemented with information from a patient questionnaire to provide its diagnoses. The innovative tool offers elderly individuals—prone to influenza—with a more comfortable, accurate diagnosis.
A Move Toward Proactive Healthcare Policies
Since revising the Pharmaceutical Act in 2014, the Japanese government has been moving swiftly to upgrade its healthcare system with digital therapeutics and implementing forward-thinking policies and initiatives. The government has launched numerous initiatives over the years to promote the adoption of electronic health records (EHRs), telemedicine, and other digital health tools.
CureApp, a startup company pioneering digital therapeutics in Japan, received Japan’s first regulatory approval in 2020 for its “CureApp SC” nicotine addiction treatment app, followed by the world’s first regulatory approval for hypertension in 2022 for its high blood pressure management application. These efforts are supported by policies aimed at creating a favorable regulatory environment for digital health innovation, including streamlining the approval process for digital health solutions and providing financial incentives for their adoption.
“In terms of demographics, there’s a good foundation for digital therapeutics in Japan to become as prevalent as that in the US,” said Naoyuki Kanda, business producer at Astellas Pharma in an interview. “When you look at specific disease areas and applications, digital therapeutics are advancing quite a bit. Two digital therapeutics are already receiving public reimbursement in Japan. When you consider all these factors, there’s big potential for the Japanese digital therapeutics market.”
Japan’s success in digital health is also attributed to the collaborative efforts between the government, private sector, and academic institutions. This collaboration has facilitated the integration of digital health technologies into the healthcare system, ensuring that innovations are effectively translated into clinical practice. Public-private partnerships are instrumental in driving the development and adoption of digital health solutions to improve healthcare—and an area in which the United States is still developing.
“Many of the APAC countries can move quicker than the US when it comes to reimbursement,” added Molnar. “Clinical trials must be done on the Japanese population for market authorization in Japan, so we are seeing large growth in Japanese companies that are focused solely on the Japanese market. And you can see this through more local associations such as JaDHA (the Japanese digital health association). Japanese companies have big international footprints as well, so this will certainly influence global markets.”
A Longstanding Cultural Acceptance
The innate cultural acceptance of technology in Japan plays a crucial role in the adoption of digital health solutions. The Japanese population’s openness to technology has enabled the rapid adoption of digital health tools, making it easier to integrate these technologies into everyday healthcare practices.
They were among the first to adopt technologies such as Nintendo’s Game Boy and Sony’s Walkman in the early 1980s, and today, Japan is a world leader in robotics where humanoid robots are commonplace in Japanese homes and workplaces, including healthcare settings. Today, the tide is turning again.
Japan’s leadership in digital health is the result of a multifaceted approach that combines technological innovation, proactive healthcare policies, and a collaborative ecosystem. By addressing its demographic challenges through digital solutions and fostering an environment conducive to innovation, Japan sets a global benchmark in leveraging technology to enhance healthcare outcomes.
As digital health continues to evolve, Japan’s experiences offer valuable lessons for other countries looking to harness the potential of technology to improve healthcare delivery and patient care.
About the Author
Dave Hanaman is co-founder, president, and chief commercial officer of Curavit Clinical Research, a virtual contract research organization (VCRO) that designs and executes decentralized clinical trials and specializing in digital therapeutics. He is a proven entrepreneur, operator, and board director. Founder of C3i, a Business Process Outsourcing (BPO) healthcare provider, Hanaman developed and led its sales, marketing, product development, and alliance strategies. He serves as a board member and advisor to several start-up and growth-stage companies in healthcare and technology. Hanaman graduated from the University of California at Berkeley and served as a deployed US Navy intelligence officer. He can be reached at dave.hanaman@curavitclinicalresearch.com
When biopharma companies test novel therapies in clinical trials, the primary focus of the research is on determining if the intervention works, with the goal of achieving FDA approval to enter the market. But there’s another part of clinical development that must not be neglected: health economics and outcomes research (HEOR), a multidisciplinary approach to evaluating the economic and clinical outcomes of healthcare interventions.
Sponsors that skip this step could develop a safe and effective novel drug but fail to effectively commercialize it because payers don’t recognize its cost/benefit improvement over existing options and do not cover it. Expensive therapies and diagnostics could therefore be out of reach for patients. Patients holding on to the promise of a new therapeutic solution are devastated, leading to negative sentiment against the sponsor. On the other hand, sponsors that demonstrate positive economic impact to payers early on could simultaneously bring their drug to market faster (without the requirement of additional studies) and to more patients at launch. Everybody wins.
Even HEOR analysis that shows financial strain provides sponsors with vital data to inform the creation of drug pricing strategies and copay assistance programs to circumvent any negative consequences. Depending on the trial phase and therapeutic area, economics data empowers sponsors to make smarter decisions around whether to modify the protocol design for future trials for additional indications or, post-FDA approval, to change their marketing strategies.
Historically, HEOR has not been prioritized because it is an additional step in an already multi-year and multi-million-dollar clinical trial process. HEOR analysis requires large amounts of data from sources such as hospitals, pharmacies and payers, which has been difficult to capture efficiently. But with the recent growth of decentralized clinical trials (DCTs), HEOR can and should be prioritized. DCTs are inherently more flexible because they are not reliant on physical sites and, therefore, can capture data virtually anywhere—and in the real world rather than an office setting, for greater accuracy.
I co-founded Curavit, a virtual contract research organization (CRO) that designs and executes DCTs, and have seen firsthand the benefits of HEOR analysis included as a natural extension of evidence generation in clinical research.
The Importance of HEOR
HEOR can play a critical role in bringing new drugs to patients by providing insights on the economic implications associated with novel therapies. The maturation of claims and health information exchanges (HIEs) now enables a cost-effective and straightforward process for drug researchers to compliantly access patients’ data. Trial sponsors can take advantage of these exchanges and leverage the data at scale for both pre-screening and health economics analysis. Another development facilitating HEOR is the accelerating acceptance of decentralized/digital trial and virtual site models that make it easier to incorporate this analysis without conducting a new, standalone study.
HEOR informs analyses of cost-effectiveness, health-related quality of life and broader analyses of the impact a new therapy can have on hospital and community clinic costs. This is particularly important with today’s shift toward value-based healthcare, which focuses on delivering the best possible outcomes for patients relative to the cost of care. Value-based care could double in value from $500 billion to $1 trillion, according to a McKinsey analysis—a powerful indication of the healthcare system’s trajectory. The rising cost of healthcare is a concern for everyone—patients, payers, practitioners and politicians. Capturing evidence of the economic value of a product, both as it pertains to individual patients and the broader population, has never been more important.
Show Me the Money: The Benefits of Using DCTs for HEOR Analysis
Jerry Maguire’s iconic line in the 1996 movie with the same name was as raw and true in the world of sports management as it is in today’s pharmaceutical world. In line with the growing use of DCTs, Curavit is seeing burgeoning interest from sponsors in health economic studies, particularly in Phase IV trials. These late-stage trials are designed to capture long-term impact data on the efficacy, durability and financial impact of an investigational drug and therefore align with a DCT model.
The advantages of using DCTs to gather HEOR data include real-world relevance: since DCTs generate evidence in diverse patient populations and settings, they reflect the complexities of routine clinical practice. HEOR leverages this data to assess the generalizability and long-term outcomes of pharmaceutical interventions, informing healthcare policy and practice.
Another plus of DCTs is faster market access. HEOR evidence expedites market access by providing stakeholders with comprehensive insights into an intervention’s value proposition, but many sponsors skip this step because it can be too daunting to gather this evidence before it goes to market. By leveraging the flexibility and efficiency of a decentralized model for research, sponsors can demonstrate cost-effectiveness and favorable outcomes to streamline not only regulatory approvals (both initial and for additional indications) but also reimbursement negotiations.
This is particularly applicable to large pharmaceutical companies that are making new investments in novel digital healthcare applications, sometimes as diagnostic tools but often as companion therapies to traditional medications. These unique digital therapeutics have been struggling to secure market access and payer coverage, but by incorporating HEOR analysis in clinical trials, sponsors can gain the evidence they need to secure coverage.
What does this look like in practice? Consider a global pharmaceutical company conducting a DCT to evaluate a novel medication for a chronic condition such as diabetes. By integrating HEOR into the protocol design, the sponsor can identify economic endpoints, such as healthcare utilization, medication adherence and quality-adjusted life years (QALYs), to assess the intervention’s current economic impact. From there, the same sponsor can develop intelligent health economic models to estimate the long-term cost-effectiveness of the intervention and broader economic impact on the healthcare system.
How to Incorporate HEOR Analysis into a DCT
Trial Design: Identify relevant economic endpoints and outcome measures. Consider the feasibility of collecting real-world data remotely, and design methodologies to capture economic and quality-of-life outcomes effectively.
Patient Recruitment and Engagement: For trials designed to study additional indications for an approved drug or extended therapeutic indications of a drug (e.g., NIH’s “DETERMINE” open label Phase II/III trial for rare cancers), HEOR analysis can help tailor patient recruitment strategies by quickly identifying target populations likely to benefit from the intervention.
Data Collection and Analysis: Incorporate economic endpoints into the DCT alongside clinical endpoints.
Invest in Knowledge for ROI
Benjamin Franklin once said, “An investment in knowledge pays the best interest.” As sponsors pour upward of $50-$150 million dollars into each Phase IV trial (not to mention the cost of earlier-stage drug development), incorporating HEOR analysis up front in a decentralized trial is like buying an insurance policy for a return on that investment. It provides not only efficacy data but also financial knowledge.
As DCTs continue to evolve, leveraging HEOR will be essential in maximizing the impact of new pharmaceutical interventions across today’s value-based healthcare environment. Make HEOR analysis a part of the protocol design from the start and continue integrating HEOR methodologies throughout the trial to enhance decision-making, improve patient outcomes and expedite market access for innovative treatments.
Joel Morse is co-founder and CEO of Curavit, a virtual contract research organization that designs and executes decentralized clinical trials.
In this video roundtable, Lokavant CEO Rohit Nambisan, Medable CSO Pam Tenaerts, and Curavit Clinical Research CEO Joel Morse discuss the increasing use of digital technology in decentralized clinical trials. In the wake of the COVID-19 pandemic, clinical researchers were driven to sourcing and enrolling trial participants in new ways, which has enabled more diverse demographics to participate. With the expanded representation of cultural minorities, our experts expect more accuracy in the growing data sets, but what other advantages are there to decentralized clinical trials? What are the obstacles and the challenges being faced in this relatively young practice? And what does the future look like? Watch our video roundtable now to find out what our experts think.
Regardless of the path to market they ultimately take, DTx companies must be poised to harness and deploy data and information that can prove their products’ economic value. Without it, the innovative treatments that they produce will continue to struggle to find success.
Over the last decade, a variety of groundbreaking digital therapeutics (DTx) have emerged to provide effective management of a range of conditions, including substance abuse, sleep disorders, depression, ADHD and more. As the population ages, DTx are poised to offer innovative and cost-effective solutions to address the inevitable increase in chronic disease that will follow.
Yet despite positive efficacy and economics, healthcare professionals have been slow to prescribe or even recommend DTx products to their patients for a variety of reasons. The lack of widespread knowledge and understanding about DTx products among clinicians, as well as complications with prescribing such therapies, administrative challenges, and insufficient insurance coverage have all created significant roadblocks for getting these potentially valuable treatments into the hands of those who can be helped by them.
Moreover, the entire process of development has been fraught with challenges as well. DTx companies often struggle to conduct clinical trials for their products because of the lack of principal investigators who have enough exposure to them. And once DTx products have proven to be effective in clinical trials, they still face the daunting challenges of FDA approval and payer reimbursement, processes rooted in an infrastructure that was designed decades ago for more traditional therapies.
Proof of economic viability offers a path forward
As a result of this wide range of obstacles, too many DTx companies that produce safe and effective products that improve outcomes for patients have been unable to achieve economic viability through traditional means. Unfortunately, this circumstance is unlikely to change in the near term. Yet a solution to this vexing problem can be found in harnessing the health economic value of DTx products.
The rising cost of healthcare is a concern for everyone—patients, payers, practitioners, politicians. Because of this, health outcomes and cost-effectiveness have become increasingly important. That means that capturing evidence of the value of DTx, both as it pertains to individual patients in certain therapeutic areas as well as their impact on the broader population, has never been more important. If companies can prove both the efficacy and the value of their products, they will ultimately improve their chances at gaining access to markets, payer coverage, and clinician and patient adoption. To be successful, DTx companies must find efficient ways to capture health economics data from day one.
Many companies are choosing to bypass payers and sell directly to employers. One example is a California-based digital health company that offers programs aimed at chronic disease prevention and management. Its services are designed to empower individuals to change their behaviors and reduce their risk of chronic disease, including diabetes prevention and management, hypertension, behavioral health, and weight management. They solved this problem by designing their programs to integrate with an employer’s existing healthcare benefits to support employees in improving their health outcomes through lifestyle changes and digital coaching.
Selling directly to employers allows digital health companies to provide their technology solutions as part of an employee benefits package, helping employers to reduce healthcare costs, improve employee health outcomes, and enhance overall workforce productivity. By offering its services as part of an employee benefits package, companies can reach a wider audience, providing personalized, scalable interventions that are accessible anytime and anywhere, which is particularly appealing for employers looking to support a healthy and engaged workforce.
HEOR will lead the way to the direct-to-patient model
Leaning into Health Economics and Outcomes Research (HEOR) offers a particularly strong opportunity for DTx companies to pivot toward directly marketing to patients themselves and away from the problematic traditional prescription model.
And while the direct-to-consumer model will certainly reduce the reliance on payers and practitioners, it is also likely to increase the need for companies to effectively prove the economic value of their products to successfully convince patients to try these novel digital therapies. In fact, the bar for demonstrating HEOR might be even higher for over-the-counter solutions to overcome any fear or distrust inherent to something unfamiliar.
With the maturation of Claims and Health Information Exchanges, which enable a cost-effective and straightforward process for researchers to gain access to identified patients’ data, trial sponsors will be able to take advantage of these exchanges at scale and leverage the data for both pre-screening and health economic analysis. And as the number of decentralized and virtual clinical trial sites grows, so will the number of trials that include HEOR evidence capture. These elements will play a crutial role in the ability of DTx companies to see success with the direct-to-patient model.
Regardless of the path to market they ultimately take, DTx companies must be poised to harness and deploy data and information that can prove their products’ economic value. Without it, the innovative treatments that they produce will continue to struggle to find success.
Joel Morse
Joel Morse is co-founder and CEO of Curavit, a virtual contract research organization (VCRO) that designs and executes decentralized clinical trials. He is an experienced operational CEO who has founded, built, and sold large global businesses in healthcare and life sciences. Previously, Morse founded C3i, a Business Process Outsourcing (BPO) healthcare provider, and built it into a global leader in tech-enabled clinical trial services, with a strategic client list that included Medidata, Quintiles, and Merck. Morse has a BS in mechanical engineering from Tufts, and an MBA from Columbia
The six steps to designing a successful diversity action plan for a clinical trial protocol.
Natalia Husby, Solutions Manager, Curavit Clinical Research
In December 2022, Congress passed the Diverse and Equitable Participation in Clinical Trials (DEPICT) Act1 which made it mandatory for sponsors to submit diversity action plans for clinical trials to the FDA early in the process. “Individuals from these populations are frequently underrepresented in biomedical research despite having a disproportionate disease burden for certain diseases relative to their proportional representation in the general population,” the agency commented.
The new legislation, along with growing industry awareness and motivation to right past wrongs, is changing the tide. While DEPICT allows for exemptions to the diversity plan requirement, trial sponsors must justify their waiver. And beginning this year, the FDA will publish, annually, an aggregate report of diversity action plans, along with the reasons any trials fell short of their set goals. This essentially creates accountability (albeit limited) for following through on diversity plans.
Some experts, however, say that the legislation doesn’t go far enough.
“Today’s policies and guidance are a start, but they should not be confused with being a mandate for diversity,” says Craig Lipset, founder of Clinical Innovation Partners and co-chair of the Decentralized Trials & Research Alliance (DTRA). “What is now required today is a diversity ‘plan,’ and the response for failure to deliver on that plan may be limited to requiring follow-up, real-world data studies. Such an outcome will only exacerbate there being a two-tiered system of evidence. There are opportunities to legislate more ‘carrots and sticks,’ as we know incentives drive action and commitment.”
Bridging the gap for small-to-mid-sized sponsors
While improving diversity in clinical trials is critical, it is not a simple endeavor—particularly for small-to-mid-sized biotechnology and startup digital therapeutics companies.
Global pharmaceutical companies have long faced the diversity issue, and in many cases, have dedicated significant time, funding, and personnel to begin to address it. Pfizer, for example, collaborated with the Tigerlily Foundation to create Health Equity Advocacy and Leadership (HEAL) workshops to better understand the breast cancer journey for women of color and foster inclusivity in clinical trials.2 The company also joined the #InclusionPledge—an initiative that aims to hold organizations accountable for taking specific actions to eliminate disparities for Black women living with breast cancer.
In addition, Johnson & Johnson is using artificial intelligence (AI) to increase diversity in 50 trials and plans to take that number to 100 in 2024, according to Najat Khan, PhD, J&J’s chief data science officer.3 The big pharma developed an internal platform called Trials360AI that leverages large de-identified datasets powered by AI and machine learning to help identify research sites with a high probability of enrolling diverse patients.
These behemoth organizations have a resource advantage and can leverage already-established diversity and inclusion programs, dedicated recruitment funding, and preexisting relationships with community outreach groups to support greater patient diversity within their clinical trials. But for other companies, the cost and logistics associated with recruiting and retaining a diverse cohort of participants can be daunting. Developing a diversity action plan adds a thick layer of up-front work that slows progress and increases costs—for instance, the expense associated with finding and engaging boutique partners who are experts in specialties such as minority recruitment.
One of the biggest challenges—for large and small companies—is retrofitting a protocol design already in progress to meet the new regulatory requirements. Not only is it time-consuming to reverse-engineer a diversity plan into an existing protocol but it’s also not always effective. Early planning is the key—even more so if the sponsor is planning on incorporating a virtual component to the trial. It is very difficult to “digitize” an existing protocol rather than building a protocol fit-for-purpose from the ground up with digital components baked in from the start.
The new FDA guidance says a diversity plan should outline the following:
Enrollment goals, disaggregated by age group, sex, and racial and ethnic characteristics.
Rationale behind these goals, including information about the condition and its prevalence among various groups.
Outreach and enrollment strategies to accomplish these goals.
Some of the key strategies sponsors can employ include limiting exclusion criteria (the FDA has acknowledged its past guidance may have led sponsors to go overboard on their inclusion/exclusion criteria and is now trying to be more flexible); embracing digital tools to identify more participants based on demographics; and reducing the burden on participants by leveraging decentralized clinical trial (DCT) methodologies and technologies, such as eConsent and virtual trial sites.
Not sure where to start? The following are six steps that follow Curavit’s inclusivity, diversity, and equity in action (IDEA) toolkit,4 which involves a clinical trial planning and support framework designed to help sponsors navigate the myriad challenges in developing and executing diversity action plans (see Figure 1).
Figure 1. A support framework for diversity action plans.
Source: Curavit
Inclusivity, diversity, and equity in action
1. Research: Conduct situational analysis. Before protocol designing, prepare a summary document consisting of information about the trial’s specific patient-population needs based on therapeutic area, disease risk factors, and potential obstacles to recruitment and retention. Conduct a thorough analysis of the demographics of the target population, looking at the latest census data while overlaying the geographic prevalence of patients with the disease being studied.
Understanding geographic prevalence provides insights on which regions to target for recruitment for investigator sites and patients while also informing any decisions around decentralization. For instance, if the patient population with the highest disease prevalence is clustered in remote areas throughout the southwestern US, an electronic consent tool and telehealth services should be built into the protocol design to reduce potential travel burdens. To understand the prevalence of this disease among different groups, it is useful to review National Institute of Health publications and CDC data.
In most cases, this preliminary research requires a few different data sources overlaid on top of one another to correlate geography with disease prevalence and demographics. Cross-reference multiple data points to ensure the accuracy of that patient population. This will give study staff a composite picture of the situation to better inform the diversity plan.
There is one caveat: because patients are historically underrepresented in research, existing data may not accurately reflect the true prevalence of the disease among minority groups. Until more accurate data is generated, consider over-enrolling across population minority groups.
2. Design: Map out a strategic diversity plan. The key word is “strategic.” The plan should be based on a thorough analysis of the demographics of the target population, including the potential barriers to participation. It must also include realistic recruitment goals, patient engagement, retention strategies, and metrics for measuring success. Seek the assistance of a specialty firm to help create this plan and enroll appropriately representative numbers of participants from underrepresented populations to be submitted with investigational new drug and investigational device applications.
3. Implement: Optimize the protocol design based on the diversity, equity, and inclusion (DE&I) plan. Once the DE&I plan is finalized, optimize the study design, taking into consideration the results of the situational analysis research. This starts with strategic site selection (if using brick-and-mortar sites) in diverse communities or identifying a combination of traditional and alternative or virtual sites that will enable the greatest access to the target patient population.
Also, talk to patient recruitment specialists to uncover innovative and new recruitment methods, technologies, and partners uniquely qualified for reaching the target patient population. If needed, adjust the protocol design to improve patient enrollment and retention across historically underrepresented groups. This may include reconsidering inclusion/exclusion criteria and eliminating any overly strict eligibility criteria.
At this point, too, consider incorporating decentralized methods and technologies into the trial design to improve patient enrollment. DCTs reduce many of the traditional barriers to study participation. For example, a DCT that uses virtual trial sites does not require travel (and the associated expense) for participants, requires less time off work, and offers more flexibility not limited by a medical office’s operating hours.
4. Engage: Review engagement materials for diverse communities. Deciding whether to participate in a clinical trial can, frankly, be a big undertaking. The risks and benefits must be weighed carefully and that is not always easy for those who may not have a high degree of health and science literacy. Having trusted friends, family, and community members to consult about the decision can make all the difference for a hesitant would-be participant. By partnering with local community organizations, leaders, and community medical providers, clinical trial sponsors can spread awareness of their studies through those who are already deeply embedded and trusted in their communities. These community leaders can help build a bridge of familiarity, trust, and understanding between the study team and potential participants.
It’s important to review recruitment content to ensure productive engagement with historically underserved communities. Avoid natural bias by seeking external feedback on the language, design, imagery, and cultural relevance of all patient recruitment marketing materials (i.e., websites, brochures, social media posts). Address any cultural and linguistic barriers to participation by translating study materials into different languages using culturally appropriate visuals and messaging, and providing interpretation services during study visits.
5. Train: Foster diversity in research teams portfolio-wide. Clinical trial sponsors should foster diversity within their research teams. This can include recruiting and promoting researchers from diverse backgrounds, providing training and support for researchers to better understand and work with diverse communities, and ensuring that study teams reflect the diversity of the population being studied. Some studies have even shown lower attrition rates of minority participants when the study teams are from familiar and similar cultural backgrounds.
By promoting DE&I internally, sponsors and sites bring unique perspectives and cultural competencies to trials. For example, a Black female research coordinator noted that a trial participant told her how thankful she was to see someone who looks like her on the study team—“it gives me a sense of community and fosters trust,” she said.
6. Monitor: Continuously check in on diversity milestones. Sponsors should be aware of the changing demographics of the study participant pool throughout the course of the study and be prepared to take steps to address any shifting gaps in representation. Track attrition rates in real time and continuously look to eliminate stress points that might be causing participants to discontinue their involvement with the trial. Technology platforms can provide study teams with near-real-time dashboards to track enrollment progress versus projected milestones to continuously monitor status and optimize as needed.
Managing diversity in clinical research is an ongoing process of fine-tuning, monitoring to see if you are hitting key milestones as outlined in the plan, and refining in a cyclical process for continuous improvement. For example, in a multi-year clinical trial that might involve more than 20,000 participants, staff should be ready to course-correct in expectation of patient attrition, as recent data shows about 18%5 and as high as 38%6 of patients drop out across therapeutic areas and phases. Further analysis5 reveals that sponsors need to identify 10 patients to randomize just one.
Given the variability from trial to trial, there’s no one-size-fits-all approach, technology, or methodology for diversity planning. However, starting with a proven framework can accelerate the planning process, remove uncertainty, and prevent costly missteps when it comes to meeting diversity milestones.
What does the future look like?
With the US government, for the first time in history, codifying into law the responsibility to ensure a representative patient population, it is a landmark moment for the clinical research industry. And while it is a long overdue one, it will take some time to get the new changes right and will require a long-term commitment.
There are no silver bullets nor sustainable quick fixes. Still, the life sciences industry is inching toward a better research environment that looks different than it did a decade ago—and that will benefit all of humanity.
Natalia Husby, Solutions Manager, Curavit Clinical Research
Along with the development of connecting technology – which has advanced even further since the COVID-19 pandemic – the concept of the decentralized clinical trial (DCT) has become increasingly popular (and successful). Digital technology enables trial sponsors to cast their nets further than ever before, inviting and including participants from more remote areas, as well as those from underrepresented cultural backgrounds. Ethnic minorities account for between 2 and 16 percent of clinical trial participants, according to Medable’s chief development officer Hady Khoury. But in this age of data, the tools used to generate a cohort of suitable participants have been disrupting conventional practices over the past three or four years. What’s next?
Accurate predictions of the future are often a result of recognizable trends being seen today, so we approached a selection of experts to generate a few ideas about what we can expect from the DCT approach in 2024. There was consensus that the “D” will eventually be omitted from the DCT acronym altogether as decentralization becomes the industry standard.
Medable CSO Pamela Tenaerts explains, “By the end of 2024, the life sciences industry won’t distinguish DCTs from clinical trials anymore […] Even with existing regulatory nomenclature, the acronym DCT will become less of a call-out as a distinct type of unique clinical trial – and that is a step in the right direction. The term suggests that a decentralized trial is uncommon and requires special extra adjustments – but that is not true. Recent guidance from the FDA and other global regulatory agencies explicitly note that decentralized trials simply need to comply with existing regulations for clinical trials – nothing extraordinary. There may be some data quality/privacy/security considerations, but the existing playbook still applies to trials leveraging decentralized innovations. By this time next year, decentralized clinical trials will simply be clinical trials (with certain parts appropriately decentralized) and the impact of this model will be much more prevalent.”
Executive general manager of customer value at Medable Alison Holland agrees: “DCT methodologies give us more options around evidence collection and opportunities for data capture in real time all with greater integrity and less friction for the patient. Now, as we ring in a new year, we are simply working to decide what elements should be decentralized to get the desired outcome. With more choices about how to package a clinical trial ecosystem, we can make research more of a consumer-like process. There is far more capacity now to connect with broader patient populations using new digital technologies […] Over the last 18 months, the industry has spent a lot of time trying to define DCTs and debating what they consist of.”
Clinical trial specialist, Curavit Clinical Research, Rachel Rangel adds, “Actionable solutions that will flourish in 2024 include: modern research models, such as DCTs that use virtual sites to meet participants where they are; partnerships with community organizations, leaders, and medical providers; diverse research teams who can better understand participants from these communities; real-time monitoring to expeditiously rectify any gaps in representation early; and, a focus on cultural linguistic barriers by translating study materials into different languages, using culturally appropriate messaging, and providing interpretation services as needed.”
Is it fair to suggest that data and data sharing will power a new revolution in connecting technologies, including AI and ML, to speed up the drug discovery and development processes? Rohit Nambisan, CEO and co-founder of Lokavant, thinks so: “Personalized medicine development will continue its fast pace in 2024, which will lead to a proliferation in data types (including an increased focus on genomic data) and more adaptive trial designs. Data collection, and, hopefully, data sharing, will take center stage – enabling us to pursue additional research questions and perform meta-analyses. Despite all the hype around AI and large language models, the key for AI success is our ability to access volumes of well-harmonized, governed, real-world data.”
Researchers are thus looking to integrate DCT methodologies into the standard toolkit, as well as in the majority of trial processes. As sponsors continue to look for new ways of engaging patients and collecting data reliably, the shift could be both transformational and wholesale. To conclude with Holland’s prediction: “Higher fidelity data collection and greater objectivity in signal detection will enable a more informed understanding of an investigational medication’s safety and efficacy.”
US-based device company Sana Health is seeking breakthrough device designation from the US Food and Drug Administration (FDA) following the completion of a decentralised trial (DCT) from virtual contract research organisation (VCRO) Curavit Clinical Research, for its Sana virtual reality (VR) device.
The Sana device is a wearable, VR mask that reduces the symptoms of post-traumatic stress disorder (PTSD) using audiovisual stimulation (AVS). The device delivers AVS in the form of coordinated pulses of light through closed eyelids, and sound at various frequencies.
The trial (NCT05319405), funded by the US Department of Defense’s (DoD) Military Operational Medicine Research Program (MOMRP), recruited more than 45 patients from a Veteran’s hospital over 28 days. The study had a 76% participant retention rate and successfully remotely monitored patients using electronic patient-recorded outcomes assessments.
PTSD, commonly observed among military personnel, is a mental health condition stemming from exposure to traumatic events during service. Symptoms include flashbacks, severe anxiety, and nightmares, significantly impacting daily life. According to the National Center for PTSD, of the six million veterans that served in 2021, 10% of men and 19% of women were diagnosed with PTSD.
The use of VR in mental health is gaining traction, with common uses including exposure therapy to treat individuals with severe phobias or obsessive-compulsive disorder (OCD).
According to a report on GlobalData’s Pharma Intelligence Center, the global VR market will reach $51bn by 2030, growing at a compound annual growth rate (CAGR) of 27% from $5bn in 2020. VR has been noted as being a promising alternative to pharmacological intervention in the therapy space, as it is cost-effective and less time-consuming for patients, healthcare professionals, and primary carers.
In the announcement accompanying the data, Sana Health CEO Richard Hanbury said: “Curavit provided us with a streamlined path to capture real-world data with the utmost professionalism, allowing us to conduct a high-quality and successful trial. Thanks to Curavit, we are moving onto a larger pivotal study, funded by MOMRP (DoD).”
Launched in 2020, Curavit designs and provides DCT execution – DCTs are trials where participants take part in the study remotely, minimising the necessity for frequent visits to a research site, and removing geographic and physical barriers to participation and execution of trials.
Curavit Clinical Research announced that its virtual trial for the Sana Device, a novel digital therapeutic aimed at easing PTSD symptoms through audiovisual stimulation, has shown promising outcomes. Involving more than 45 participants from a Veteran’s hospital, the study not only achieved a commendable 76% retention rate but also marked a pivotal advancement in mental health treatment methods, with the data now under FDA review for Breakthrough Device Designation.
Leveraging its expertise in decentralized clinical trials (DCTs) for digital therapeutics (DTx), Curavit Clinical Research has made strides in mental health treatment with the Sana Device. This wearable, virtual-reality-style mask employs audiovisual stimulation for on-demand anxiety relief, specifically targeting symptoms of post-traumatic stress disorder (PTSD).
The success of this innovative therapy has led to the submission of trial data to the U.S. Food and Drug Administration (FDA) for Breakthrough Device Designation consideration, showcasing the potential of digital interventions in modern healthcare.
Richard Hanbury, CEO of Sana Health, highlighted the potential of the Sana Device to assist patients with pain and mental health issues, stating, “The Sana Device has tremendous potential to help patients with pain and mental health issues, but we needed a more efficient, modern way to study and demonstrate efficacy and safety.”
More than 45 patients from a Veteran’s hospital participated in the 28-day study. Curavit exceeded Sana’s expectations for participant retention with a 76% retention rate. The trial was managed remotely, with all aspects of participation overseen by remote-based clinical research coordinators (CRCs), a remote-based principal investigator, and a comprehensive technology platform that included ePROs, eCOA, telehealth, device training, and randomization.
Curavit CRCs documented participants’ experiences with the Sana Device using the industry-standard PHQ-9 survey and the Columbia Suicide Severity Risk Scale (C-SSRS) to assess levels of depression—all conducted remotely through electronic patient-reported outcomes assessments.
The Sana Device is designed to provide anxiety relief on demand. The trial aimed to collect evidence of the device’s capability to offer additional relief to patients suffering from PTSD while they are on waiting lists for further specialty care. In 2021, the Sana Device received FDA Breakthrough Device Designation for the treatment of Fibromyalgia.
“Real-world evidence is crucial for DTx companies to secure insurance coverage and reimbursement by demonstrating to payers and providers the full impact of these innovations. Curavit’s HEOR services generate the real-world data required to unlock wider coverage and greater availability for transformative digital treatments,” added Andy Molnar, CEO of the Digital Therapeutics Alliance (DTA).
The successful trial represents a significant milestone in the treatment of mental health disorders, offering a glimpse into the future of non-invasive, accessible therapeutic options. Curavit has recently introduced its Health Economics and Outcomes Research services to gather evidence on the economic value of novel pharmaceutical products, with a particular focus on digital therapeutics.
We asked members of DIA’s scientific and publications communities to share their predictions for the life sciences in the coming year. All responded creatively, although some responded anonymously. We hope you enjoy reading these predictions now AND revisiting them later to see how many came true in 2024.
AI in Patient and Professional Engagement
AI for patient and healthcare professional engagement is booming, but expect stricter rules in 2024:
Federal, state, and private watchdogs will check AI not only for accuracy, but also for fairness and bias.
Data privacy as applied to AI will get serious attention from regulators.
It will become more important to be able to explain how AI works, source the results, and explain what the AI finds.
Lawsuits will begin to be filed over AI mistakes. Some of these lawsuits may result from patients and healthcare professionals feeling targeted, and then worried about data privacy. This will result in a loss of trust.
If AI is done legally and compliantly, especially by sales and medical information personnel, trust can be built into the system. While FDA has focused on Quality by Design, AI lawyers will need to work with sales and medical affairs teams to build trust by design into the systems. — Darshan Kulkarni, Kulkarni Law Firm.
The Competitive Pharmaceutical Landscape
The competitive pharmaceutical marketplace will compel increased trial innovation: The pharmaceutical marketplace is more competitive than ever, particularly in the race to be first-to-market. For instance, the time between the first FDA approval for a vaccine for the respiratory ailment RSV to the fourth FDA approval for a similar vaccine was less than six weeks. The first-mover advantage is dramatic, so clinical trial sponsors need to be focused on maximizing every second and not wasting time. To that end, large pharmaceutical companies are setting lofty goals of 50 percent reductions in cycle time next year, which means that the status quo won’t allow them to reach such significant new goals. Sponsors will need to make commensurate changes to accelerate drug development. Decentralized clinical trial (DCT) methodologies will become part of the standard toolkit, embedded into most trial processes and operational decisions, because sponsors need new ways to collect data reliably and engage with patients in a competitive marketplace. In 2024, the shift to DCT methodologies will be transformative and wholesale, bringing DCT elements into the organization at the portfolio level rather than trial by trial. DCT methodologies allow for higher fidelity data collection and greater objectivity in signal detection, removing skews and biases. This enables a more informed understanding of an investigational medication’s safety and efficacy, which allows companies to reduce the sample size—and fewer participants means less patient recruitment time and lower costs. One major multinational pharmaceutical company reduced its sample size by 70 percent this way, helping to speed drug development and time to market. — Alison Holland, Medable.
Data Sharing and Cross-Industry Collaboration
Data sharing and cross-industry collaboration will power the 2024 AI revolution in clinical research. No one company has enough data to drive accurate productions around a single disease or use case, which is why cross-industry collaboration like we witnessed during the pandemic will be reinvigorated. During COVID-19, pharmaceutical companies, clinicians, researchers, technology companies, and regulators worked together in harmony. The MELLODDY trial provides a current example of how this can work: MELLODDY is using federated learning, a data-sharing model that protects companies’ proprietary information while still sharing important research data, to provide much-needed, high-quality protein data to help AI/ML models design proteins faster. Protein drug development is notoriously long, arduous, and costly. However, organizations contributing to the MELLODDY trial can use AI to adopt generative biology and are experiencing greater efficiency than any individual organization could alone. Without this level of collaboration, AI won’t work, because it won’t provide tangible ROI and so investment (and adoption) will slow to a trickle. — Rohit Nambisan, Lokavant.
Market Access Models for Digital Therapeutics (DTx)
Digital therapeutics (DTx) companies will continue to pivot away from prescription models. In 2023, one major DTx company filed for bankruptcy and another abandoned the prescription business model. Both DTx companies raised hundreds of millions of dollars by going public in special-purpose acquisition company (SPAC) transactions. While each company successfully gained FDA approvals, current market acceptance for prescription digital therapeutics is low and improvement may take years. Given this, many DTx companies will pivot away from the prescription model and go straight to consumers in 2024. They will continue to run clinical trials to confirm their claims and value proposition but will not seek FDA approvals. — Joel Morse, Curavit Clinical Research.
DCTs: Evidence versus Hypotheses and New Focus on “How”
Evidence will replace hypotheses in DCTs: By the end of 2024, the life sciences industry will replace hypothetical surveys about the impact of decentralized methodologies in clinical research with hard evidence. The Tufts Center for the Study of Drug Development has formed a pre-competitive consortium of more than 50 companies that will collate metrics to understand how decentralization impacts protocol performance such as cycle times, patient recruitment, and retention rates, with the goal to publish its first data set by spring 2024. The consortium will conduct a granular analysis of actual data to gain a better understanding of the impact of specific clinical trial innovations to better inform future protocol design. With this information, industry can take a more fit-for-purpose approach for determining how to incorporate decentralized elements into more trials. With more evidence, we can get better at matching decentralized innovations to populations, diseases, and specific study designs. This could have the add-on effect of decreasing complexity: For instance, trying to implement electronic clinical outcome assessments (eCOAs), wearables, and home-health nurses in the same trial may be overkill; instead, we can carefully pre-plan to use just the technologies that are most likely to improve outcomes. As we continue to capture evidence of DCT value, we will increasingly adopt a nuanced approach, but this progression will move at the pace of maturity of each DCT innovation. — Pamela Tenaerts, Medable.
We will stop focusing on the “what” of decentralized trials and focus on the “how”: Industry has been spending a lot of effort trying to define DCTs and debating what a DCT consists of; now, we focus on their outcomes. DCT methodologies give us more options around evidence collection and more opportunities for data capture in real time—all with greater integrity and less friction for the patient. In 2024, we will simply work to decide which elements should be decentralized to get the desired outcome. With more choices about how to frame and package a clinical trial ecosystem, we can make research a more consumer-friendly process. — Alison Holland, Medable.
The acronym “DCT” will disappear as decentralization becomes the norm: By the end of 2024, the life sciences industry won’t distinguish DCTs from “simple” or “traditional” clinical trials anymore. As noted by the FDA, the modernization of clinical trials is ongoing. In the US, it will require an act of Congress to change the definition of clinical trials because the term DCT is used in provisions published by the Food and Drug Omnibus Reform Act of 2022 (FDORA), which amended the Federal Food, Drug, and Cosmetic Act and the Public Health Service Act. Other regulators are already talking about trials with decentralized elements (i.e., EMA’s recommendations paper) instead of DCTs. Even with existing regulatory nomenclature, the acronym DCT will become less of a callout as a distinct type of unique clinical trial, which is a step in the right direction. The term suggests that a decentralized trial is uncommon and requires special extra adjustments, but that is not true. Recent FDA and other global regulatory agency guidances explicitly note that decentralized trials simply need to comply with existing regulations for clinical trials—nothing extraordinary. There may be some data quality/privacy/security considerations, but the existing playbook still applies to trials leveraging decentralized innovations. By the end of 2024, decentralized clinical trials will simply be clinical trials (with certain parts appropriately decentralized) and the impact of this model will be much more prevalent. — Pamela Tenaerts, Medable.
Generative AI Coupled with Quantum Computing
Generative AI coupled with quantum computing applied to the sciences: Whether it be novel drug candidates to bioprocess improvement, the impact is now just beginning. When AI is powered by quantum computing, it will accelerate the sciences in ways that are hard to imagine. — Clark Golestani, C Sensei Group LLC.
Health Economics and Outcomes Research (HEOR) in DCTs
Health economics and outcomes research (HEOR) will become more common in DCTs. In 2023, we saw the maturation of Claims and Health Information Exchanges, which enable a cost-effective and straightforward process for researchers to gain access to identified patients’ data. Given the improvements in costs, trial sponsors can now take advantage of these exchanges at scale and leverage the data for both pre-screening and health economic analysis. As DCTs and virtual site acceptance accelerate, a knock-on effect will be that more of these trials will include HEOR analysis. — Joel Morse, Curavit Clinical Research.
Improving Local Production Capacity and Access in Latin America
In Latin America, with new governments taking office in key countries, the private sector faces changes in the healthcare agenda and policy priorities, as well as budgeting maneuvers—all complicating market access. This might bring more focus to the discussion on alternative and sustainable models for health financing. Brazil might provide a good example which offers some degree of stability, policy continuity, and many interesting opportunities for the private sector including the Waitlist Reduction Program, the Growth Acceleration Program, the Health Economic-Industrial Complex, and other government initiatives. The 2023 debate around improving capacities for local production of pharmaceutical products will continue in the 2024 agenda. — Anonymous.
Pharmacovigilance Guidelines: Remote Audits and Inspections
Most audits and inspections in the pandemic had transitioned from onsite to remote, and the transition back to onsite versions began in early 2023. With global armed conflicts and geopolitical unrest continuing or even intensifying in 2024, it is likely that regulatory inspections and routine audits will continue in remote mode. The only difference will be the addition of newer technologies to support remote assessments, and more countries would develop new pharmacovigilance guidelines or revise existing ones to reflect this remote mode. — Manoj Swaminathan, Biorasi.
Diversity in Clinical Research Participation
Participant diversity in clinical research will become a bigger priority: For 2024 and beyond, the focus on patient diversity in clinical trials will increase. The difficulties of a lack of patient representation in clinical research surfaced during the pandemic’s vaccine trials, and that issue isn’t going away. Some of our approaches may change based on what we have learned—for instance, there is far more capacity now to connect with broader patient populations using new digital technologies. Given the convenience of these tools, more patients who become increasingly comfortable with technology will take advantage of digital opportunities to connect to a trial and remain engaged through to the end. This will also help ensure patient compliance for the full duration of a trial even when patience and perseverance start to wane in the later weeks and make it harder to capture consistent data. — Alison Holland, Medable.
While industry is moving in the right direction, racial and ethnic minorities still only account for 2 percent to 16 percent of clinical trial participants while comprising 39 percent of the US population. One of the biggest obstacles is patient recruitment and retention from historically underrepresented populations. That’s why some sponsors are starting to collaborate with partners that specialize in diverse patient recruitment to carefully plan and execute new strategies that reduce some of the traditional barriers to study participation and are more conducive to reaching a broader demographic. Actionable solutions that will flourish in 2024 include modern research models such as DCTs which use virtual sites to meet participants where they are; partnerships with community organizations, leaders, and medical providers; diverse research teams who can better understand participants from these communities; real-time monitoring to expeditiously rectify any gaps in representation early; and a focus on cultural linguistic barriers by translating study materials into different languages, using culturally appropriate messaging, and providing interpretation services as needed. — Rachel Rangel, Curavit Clinical Research.
Personalized Medicine Development
Personalized medicine development will continue its fast pace in 2024, which will lead to a proliferation in data types (including an increased focus on genomic data) and more adaptive trial designs. Data collection and (hopefully) data sharing will take center stage in 2024, enabling us to pursue additional research questions and perform meta-analyses. The key to success for AI and Large Language Models is our ability to access volumes of well-harmonized, governed, real-world data. With more personalized approaches, clinical trials grow more complex—again requiring better modeling and data collection plus a reliance on modern-day data engineering and data scientists to identify trends and understand the causality of the therapeutic interventions in question.
Side effects of the pandemic will continue to unfold in 2024, as well. We will see more remote monitoring of patients and adoption of more digital health technologies, including mobile apps and specialized devices. Collecting and gaining insights from these data sources, coupled with the continuing trend of distributed clinical trials, will require data strategies from both sponsors and CROs that leverage cloud computing and data governance at a much different scale than today. — Andreas Matern, Lokavant.
Zero-Knowledge Proofs
Zero-knowledge proof (ZKP) technologies allow the independent verification of the computational integrity of any transaction or operation without any additional information. This transformational technology is exploding in Web3 and is rapidly aligning to use cases across global industries. While this cryptography isn’t new, recent research advancements have enabled “Turing complete zero knowledge proofs” to open a new world of opportunities. ZKPs enable trust-minimized applications that cryptographically enable privacy-preserving, multiparty supply and asset tracking, private verifiable machine learning models, and zero-leak data privacy to enable regulatory use cases. The biopharmaceutical industry has been advancing thought leadership and investing in distributed and multiparty operations use cases. However, the problems of interoperability, privacy, and scalability have limited their progress and impact. Zero-knowledge proofs provide a direct solution to these issues by providing all stakeholders the ability to securely validate transactions, authenticate identities, and seamlessly collaborate and automate across networks at scale, all while maintaining control and privacy of intellectual property.
In connecting the pharmaceutical supply chain, consortium-based solutions have largely failed. ZKPs can simplify interoperability between private manufacturers, distributors, and pharmacies to eliminate the risk of interparty fraud or process errors. This end-to-end traceability and verifiable process compliance can be aggregated and provided as proof to counterparties, regulators, and consumers without giving them access to private software systems and data. In clinical research, ZKPs can streamline trials by preserving patient privacy while expanding secure access to data between sites, outcomes which serve to increase trust in sharing health information, study participation, and data exchange—all accelerating pharmaceutical research progress. Zero-knowledge proof innovations from PharmaLedger and Toposware are poised to have a major impact across the biopharmaceutical industry research, commercial operations, and supply chains for forward-thinking organizations. — Clark Golestani, C Sensei Group LLC.
As advanced therapies and patient perspectives strengthen their foothold in R&D, pharma is poised to deliver impactful treatments in record time.
This is the second installment of a two-part series previewing pharma’s year ahead. Our first part examines how industry leaders see the financial market taking shape in 2024.
It’s an exciting time to be in the business of drug innovation.
The recent arrival of the world’s first approved CRISPR-based therapy has helped solidify the gene therapy movement and pave the way for more gene editing approaches. Other cutting-edge modalities such as cell therapies, antibody-drug conjugates and a new wave of RNA-based treatments are offering drug developers transformative tools for bringing more effective treatments — and even cures — to some of the world’s toughest diseases and conditions.
The continuing rise of the patient voice and emphasis on DEI are also poised to help the industry create impactful medicines in the coming years.
And as innovations around AI, data analysis and machine learning become more deeply embedded in these efforts, drug discovery and development is reaching groundbreaking levels of speed and efficiency.
It’s no surprise that when we asked industry leaders to submit their outlooks for 2024, these themes were a common thread. Here’s how they see these trends translating into meaningful industry change in 2024.
Trends in drug innovation
More antibodies will come to market
Permission granted by Genmab
“The growth of new modalities such as antibody-drug conjugates, bispecific antibodies, and cell and gene therapies, are already making a larger presence in the investigational pipeline. The focus on these novel therapies indicates a move towards addressing previously difficult-to-treat diseases, including advanced cancer and rare diseases. With hundreds of antibodies undergoing pre-clinical and clinical development, it is anticipated that the number of antibody medications in clinical trials and approved by regulatory agencies will rise.” Tahi Ahmadi, executive vice president, chief medical officer, head of experimental medicines, Genmab
Cell and gene therapy development will become more streamlined
Permission granted by Revvity
“With over 500 new cell and gene therapies entering clinical trials annually [and] their expedited time to market … this class of therapeutics [is positioned] for significant prominence. As we approach 2024, the prospect of witnessing a surge in approvals becomes increasingly imminent. Concurrently, the FDA’s proactive initiatives to bolster the advancement of these therapies promise to usher in a new era of standardization. Expectations include the streamlining of manufacturing processes, consolidation of protocols for testing Critical Quality Attributes, refined approaches to patient identification and enrolment and the evolution of companion diagnostics.” Michelle Fraser, head, cell and gene therapy, Revvity
Delivery tech will push gene therapy into new space
Permission granted by Lexeo Therapeutics
“The gene therapy environment has evolved rapidly and we are now seeing expansion into novel therapeutic areas like cardiovascular diseases, such as cardiomyopathies with genetic markers of disease. Innovation in delivery technology will continue to enable this shift, particularly AAV technology given the high transduction efficiency in cardiomyocytes, but we also predict advancement of novel delivery systems. At the same time, there has been a material shift in the regulatory landscape for both gene therapy and cardiovascular disease, with precedents now utilizing biomarkers as pivotal study endpoints as opposed to historical standards related to mortality and survival.” R. Nolan Townsend, CEO, Lexeo Therapeutics
R&D will target the underlying causes of aging
Permission granted by AbbVie
“Aging is the one health condition that has a prevalence rate of 100%. As a result, we are going to see more interest in how to address the underlying causes of aging to preserve vitality, mobility and physical appearance. This will lead to next-generation research and treatments that incorporate the underlying causes of aging versus merely addressing the signs and symptoms of the aging process to support health and longevity.” Carrie Strom, senior vice president, AbbVie; president, Global Allergan Aesthetics
Next-generation mRNA is coming
Permission granted by CSL Seqirus
“As we move forward into 2024, we anticipate a continued focus on innovation in vaccines and with that, an interest in some of the newly emerging technologies such as self-amplifying mRNA (sa-mRNA). There is an ever-present need for flexible, effective vaccine technology and as demonstrated during the COVID-19 pandemic, mRNA technology can facilitate rapid and scalable vaccine development and distribution. The sa-mRNA technology adds to these benefits by offering the potential for stronger immune responses and longer duration of protection, while using significantly lower doses compared to conventional mRNA vaccines.” Stefan Merlo, vice president, commercial development, CSL Seqirus
The obesity space will quickly evolve
Permission granted by Rivus Pharmaceuticals
“Obesity is the primary driver of metabolic diseases and, in 2024, will still account for more morbidity and mortality than all cancers combined. In 2024, we will continue to see the expansion of GLP-1 and other incretin-based approaches as the broader obesity market continues to grow. As we think about next generation approaches to treating metabolic diseases, there is a need to focus on molecular targets with new and alternate mechanisms, including those that work by safely increasing the metabolic rate. I also anticipate that machine learning and AI will play a critical role in the field, including in identifying new small molecules in a faster and more efficient way.” Dr. Jayson Dallas, CEO, Rivus Pharmaceuticals AMR investments will tick up
Permission granted by Shionogi
“We predict a return to investment in antivirals and antibiotics to address current and future medical needs. COVID-19, the flu and RSV aren’t going away and the chance of getting sick with even one of these viruses is high. We need to start actively addressing the largely silent threat of antimicrobial resistance, which could cause up to 10 million deaths by 2050 according to the United Nations. New viral threats could emerge at any time, leading to future pandemics.” Margaret Borys, senior vice president, chief commercial officer, Shionogi
More R&D will incorporate patient voices
Permission granted by UCB
“In 2024, I expect our work in early research to be even more patient-centric. It’s vital for those who research and develop medicines to listen to and engage with people impacted by severe diseases, and go further by deep investigation into the pathways driving their disease using relevant disease models. We must meaningfully consider their lived experiences in the earliest stages of R&D to ensure we are developing medicines [that] positively change the way people are living with severe disease and focus on addressing the root biological causes of these conditions; these go hand in hand. This means connecting our research teams with people and their caregivers living with the conditions we’re researching.” Roger Palframan, head of U.S. research, UCB
Maternal health innovation will gain steam
Permission granted by Organon
“The maternal health crisis continues to pose serious risks for moms-to-be across the U.S. This unfortunate reality is particularly dangerous for Black women, who are three times more likely than white women to die from pregnancy-related complications. New initiatives inspire hope that 2024 will mark a turning point. For instance, innovations are coming to the fore … like the creation of an artificial womb, which the FDA is exploring as a potential approach to help premature babies survive. The White House’s ‘Birthing Friendly’ Hospitals Initiative is [also] an important step towards helping women find high-quality maternal care. And … the WHO is working alongside key public and private stakeholders on a solutions-driven, strategic roadmap to … improve maternal health outcomes. These developments create positive momentum … to address critical gaps in maternal health.” Colby Holtshouse, global medtech commercial lead, Organon
Cancer care advances
More emphasis in oncology will be on early detection
Permission granted by AstraZeneca
“We know that the earlier we can detect and address cancer, the closer we may be to better outcomes. In the new year, I expect we’ll see a continued shift to earlier detection and intervention, both through improved access to cancer screenings and beginning treatment sooner in one’s cancer journey, as well as a supportive infrastructure that enables patient access to innovation and resources.” Mohit Manrao, senior vice president, head, U.S. oncology, AstraZeneca Successful oncology launches will be driven by tech
Permission granted by Takeda Oncology
“Digital and technological advancements will continue to accelerate in 2024. It will be up to us to responsibly leverage these tools to meet the needs of patients and providers more effectively. This will be particularly crucial for oncology companies to advance innovative R&D and optimize the delivery and use of new medicines. I predict the success of future product launches will be partially measured by the ability of developers to integrate digital processes into every step of delivering care — helping us solve potential challenges that may arise, increasing accessibility to a variety of patient populations, and eliminating barriers to care.” Stefanie Granado, head, U.S. oncology business unit, Takeda Oncology Strides will be made with tough-to-treat cancers
Permission granted by Apollomics
“The industry is gearing up to address the persistent challenges of hard-to-treat and treatment-resistant cancers. For example, although PD(L)-1 inhibitors have demonstrated effectiveness for numerous NSCLC cases, certain forms of NSCLC don’t respond. In addition, resistance develops in patients who initially respond to certain therapies. To address this, companies are directing efforts toward these challenging forms of the disease, striving to provide better outcomes for all patients. With an emphasis on cutting-edge technology platforms and robust drug development portfolios, the sector is poised for substantial progress in 2024. The integration of sound mechanistic and scientific rationale in clinical trials, exploring both monotherapy and combination approaches, reflects a significant leap toward conquering difficult cancer types.” Guo-Liang Yu, CEO, chairman, Apollomics
The tech effect
The data analyst role will evolve
Permission granted by Phastar
“As more AI-based solutions are embedded into our workflows in 2024, it will fundamentally change the role of the data analyst. We have already seen the beginnings of an evolution from data management to data science, but fundamental questions remain. Next year, we expect the discussion to focus on how analysts can learn and progress when entry-level work and data sorting is performed by a machine, how to strike the appropriate balance between AI and human insights, and how to communicate algorithm-based decisions to various research stakeholders.” Graham Clark, CEO, Phastar Generative AI will transform healthcare
Permission granted by UCB
“We’ve been talking about AI for some time, and 2024 will be the year that testing and unleashing generative AI will create value in healthcare to enable patients to live their best lives in ways that work for them individually. Based on a well-thought-out and executed overall data strategy, data-powered and data-providing initiatives will continuously inform the individualized next step for each eligible patient. The power of predictive algorithms will coordinate personalized care, from diagnosis to treatment, to find the right resources, technology and solutions at the right time. With data, we can finely tune our knowledge of patients’ individual journeys, zeroing in on their specific needs.” Kim Moran, senior vice president, head, U.S. rare diseases, UCB
Regulatory shifts
The biomarker push will remain strong
Permission granted by Ultragenyx Pharmaceutical
“We have seen an industrywide push for the FDA to provide additional guidance and support to advance gene therapies for rare and ultra-rare diseases, and this will remain a constant theme in the upcoming year. There is a clear appetite from agency leadership, but we need to see this reflected in the review divisions with more consistency. Bipartisan support from Congress has empowered the agency to adapt its policies to keep pace with innovation, but in order to effect change the agency needs to shift to a nimbler approach and place the people living with degenerative rare diseases at the crux of decision-making.” Dr. Emil Kakkis, CEO, Ultragenyx Pharmaceutical
The drug discount system will need a reboot
Permission granted by Kalderos
“The drug discount market will continue to see unprecedented growth in 2024 from the 340B program and Medicaid Drug Rebate Program, along with commercial rebates. This raises questions about the ability of drug discount stakeholders, such as drug manufacturers, covered entities, and state Medicaid agencies to handle that extra volume. We’re at the point where the entire drug discount system needs to be redesigned or it will collapse under the weight of its own complexity and lack of coordination. Next year we can expect drug manufacturers to push for changes that will mitigate the impact of regulatory control and program complexity while helping to reduce revenue bleed from duplicate discounts, which result in higher drug prices for consumers.” Angie Franks, CEO, Kalderos
Clinical trial transformations
DEI will drive innovation
Permission granted by Merck & Co.
“As we approach 2024, the landscape of diversity, equity, and inclusion in clinical trials is on the brink of a transformative shift, and I envision a future where DEI is not a mere checkbox but a catalyst for groundbreaking advancements in medical research. The industry is moving toward a collective commitment that aims to dismantle historical barriers and address social determinants of health, acknowledging and rectifying the health disparities experienced by people from marginalized groups. Through these intentional efforts, the industry can anticipate more robust and reliable research outcomes that are not only equitable and inclusive but ultimately more impactful for all.” Adrelia Allen, executive director, clinical trial patient diversity, Merck & Co.
Patients will inform trial design
Permission granted by International Drug Development Institute
“2024 will be the year of patient-driven trial design. We are already seeing the adoption of new solutions integrating multiple, study-specific efficacy and safety criteria into a single aggregated measure. This will estimate the net benefit of treatments which will help improve the clinical pertinence of trials and can minimize their sample size — on average by 20%.” Marc Buyse, founder, International Drug Development Institute
Removing financial barriers to research will become a priority
Sam Whitaker, CEO
Permission granted by Mural Health
“Next year, we hope to see a heightened focus in the industry on removing financial barriers to clinical trial participation — barriers that disproportionately affect people from lower socioeconomic and minority groups and result in a lack of diversity that threatens the efficacy of the drug development process. Clinical trial payments should be tax free, participants should have a choice in how they receive their funds and monthly inactivity fees must become a thing of the past.” Sam Whitaker, co-CEO, co-founder and Jason Dong, co-CEO, co-founder, Mural Health
A new phrase will shape clinical trials
Permission granted by Andaman7
“’Patient-mediated research’ will be the buzzword of 2024. With decentralized clinical trials (DCT) and increased ability to leverage insights from real-world data sources such as electronic health records (EHR) from hospitals and patient-reported outcomes (PROs), drug developers now have a direct line to the patients they seek to serve. By utilizing this connection and working closely with patient advocacy groups and innovative tools built by patients with lived experience, they have an opportunity to set up and conduct trials faster and collect richer data.” Vincent Keunen, CEO, founder, Andaman7
DCTs will become standard
Permission granted by Medable
“The acronym ‘DCT’ will die away as decentralization becomes the norm. As noted by the FDA, the modernization of clinical trials is an ongoing evolution. In the U.S., it will require an act of Congress to change the definition because the term DCT is used in provisions published by the Food and Drug Omnibus Reform Act of 2022 (FDORA) that amended the Federal Food, Drug, and Cosmetic Act and the Public Health Service Act. Even with existing regulatory nomenclature, the acronym DCT will become less of a call-out as a distinct type of unique clinical trial — and that is a step in the right direction. By this time next year, decentralized clinical trials will simply be clinical trials (with certain parts appropriately decentralized) and the impact of this model will be much more prevalent.” Dr. Pamela Tenaerts, chief scientific officer, Medable
Informed consent will become easier
Permission granted by Verily
“Next year, we’ll see renewed, cross-industry focus on informed consent frameworks for clinical research study participants — with a particular focus on transparency, trust and explaining how different sources of data are used for research. Instead of long consent forms that patients skip over, we’ll begin to see consent broken down into smaller steps, so patients can decide what they give permission for, for example, permission to recontact, or to link their data from different sources. The technical ability to capture these permissions in metadata will become an important part of data stewardship.” Amy Abernethy, president, product development; chief medical officer, Verily
Talent will stay competitive
Permission granted by Thermo Fisher Scientific
“In 2024, as the clinical research industry explores options to speed up its development pipelines and decrease cost, many will be looking to further migrate toward functional service provider (FSP) outsourcing models, in both the traditional and hybrid approaches. As such, we expect the sourcing of clinical development talent for client engagements to remain highly competitive. To help address this situation, large CROs that provide both full-service outsourcing (FSO) and FSP solutions … will be best positioned to deliver traditional FSP talent deployment.” Les Enterline, senior vice president, FSP therapeutic unit head, PPD clinical research business, Thermo Fisher Scientific
Two key strategies will help diversify trials
Permission granted by Walgreens
“In 2024 and beyond, clinical trials will see a renewed commitment towards more structured inclusivity and equity in trial recruitment, diversifying based on race and location (urban vs. rural). Expect a dual strategy to accomplish this: AI for rapid patient population identification and a community-centric approach to address historical fears and mistrust in certain communities towards clinical trials.” Ramita Tandon, chief clinical trials officer, Walgreens
Trials will feel the need for speed
Permission granted by Medable
“The pharmaceutical marketplace is more competitive than ever, particularly in the race to be first-to-market. The first-mover advantage is dramatic, so clinical trial sponsors are hyper-focused on making sure they are maximizing every second. To that end, large pharmaceutical companies are setting lofty goals of 50% reductions in cycle time next year — meaning, the status quo won’t allow them to reach significant new goals. Sponsors will need to make commensurate changes to accelerate drug development. DCT methodologies will be part of [that] standard toolkit.” Alison Holland, executive general manager, customer value, Medable
Better data analysis will be a side effect of DCTs
Permission granted by Curavit
“Health Economics Outcomes Research (HEOR) will become more common in DCTs. This year we saw the maturation of Claims and Health Information Exchanges, which enable a cost-effective and straightforward process for researchers to gain access to identified patients’ data. Given the improvements in costs, trial sponsors can now take advantage of these exchanges at scale and leverage the data for both pre-screening and health economic analysis. As DCTs and virtual site acceptance accelerates, a knock-on effect will be that more of these trials will include HEOR analysis.” Joel Morse, CEO, co-founder, Curavit Clinical Research
LifeSciencesIntelligence explores the primary goals of mergers and acquisitions in the life sciences industry with insight from three experts.
– Mergers and acquisitions (M&A) play a critical role in the healthcare industry. As more products come to market, companies can leverage M&A to elevate their position in the market. The value of mergers and acquisitions in the pharmaceutical industry is understood and echoed across life sciences acquisitions.
LifeSciencesIntelligence spoke to three industry leaders to understand the existing M&A landscape and what to expect moving forward: Daniel Chancellor, Director of Thought Leadership for Evaluate (a Norstella company); Gadi Saarony, CEO of Advarra; and Joel Morse, CEO and Co-Founder of Curavit Clinical Research.
OVERVIEW OF M&A IN LIFE SCIENCES
Understanding the mergers and acquisitions landscape is critical for companies in the industry. Life sciences companies must stay current on the significant players, stakeholders, and trends to understand their competition and evaluate their M&A plan.
Throughout 2023, many significant deals were propelling the M&A landscape in the life sciences industry.
“There’ve been some very clear, big deals,” Saarony began, describing the landscape. For example, “Look at Pfizer and Seagen— that’s a huge deal. It was a $43 billion deal size.”
Seagan is a sought-after pharmaceutical company, with other major players, including Merck, eyeing it before Pfizer staked its claim.
However, the company comes with an unmistakable, hefty price tag. According to the press release, Pfizer intends to finance the acquisition through $31 billion in new long-term debt.
Despite the cost of this deal, Pfizer presumably believes in the value of Seagan’s portfolio, which manufactures three oncology drugs and commercializes an additional medication. Pfizer revealed that the agreement will help expand its oncology portfolio and bolster its position in that therapeutic area.
Saarony also highlighted some acquisitions by Merck, Astellas, and Novartis, indicating that large pharma has been buying smaller and mid-size players. He explained that the investments have not focused on one particular therapeutic area but span various therapeutic areas, modalities, and technologies.
“Large pharma [companies] have to fill gaps in their portfolios, and they’re going after what’s complementary to what they have or a new space they want to get into,” Saarony added.
For example, the Pfizer–Seagan deal will complement Pfizer’s existing oncology portfolio and help expand it, providing the company with a broader reach. The company identifies Seagan as a powerhouse in the antibody–drug conjugate (ADC) space, facilitating one-third of the 12 FDA-approved ADC.
More specifically, they manufacture Dcetris (brentuximab vedotin), Padcev (enfortumab vedotin), and Tivdak (tisotumab vedotin) while commercializing Tukysa (tucatinib).
However, the life sciences mergers and acquisitions (M&A) landscape is evolving to accommodate changing practices, economic pressures, and discoveries. Although the volume of acquisitions in 2023 was greater than in 2022, it hasn’t kept up with peak years.
According to Evaluate’s quarter 3 (Q3) roundups, Q3 of 2023 had the lowest number of biopharmaceutical M&As since Q2 in 2021, with only 24 total transactions. Evaluate projects that M&A activity will be around $150 billion this year. Meanwhile, Leerink Partners estimates that healthcare M&As in 2023 will be valued at $181 billion, with biopharmaceuticals accounting for 33% of deals and 58% of the deal value.
These variations may depend on the definition of the industry. However, Chancellor maintains, “This is an increase from 2022, although it’s around the average of previous years — some of which have seen some huge industry consolidation deals.”
Even though the M&A landscape has seen a lot of variety, Chancellor identifies trends that have played a critical role in M&A. He revealed that most acquisitions are focused on late- or commercial-stage biotech companies with complementary product portfolios with the acquiring organization.
Chancellor notes that the highest demand is for companies with first-in-class drugs for newer oncology and immunology targets. Leerink Partners estimates that oncology is the most active and valuable therapeutic area, with 11 deals this year. The value of these deals is an estimated $49 billion, including the $43 billion Pfizer–Seagan deal. Comparatively, immunology was the third most active area, accounting for 7 contracts valued at $25 billion.
Beyond that, there has been a significant focus on rare diseases. Although rare disease mergers and acquisitions were more active than immunology, with 9 deals, they are valued lower than immunology transactions at $13 billion.
A prime example is the recent Roche announcement that revealed the company’s plans to acquire Carmot Therapeutics and its clinical-stage obesity drug portfolio. Although the deal is in its early stages, the company estimates that $2.7 billion will be paid upfront, and an additional $400 million may be spent through milestone payments.
Benefits of M&A
The experts told LifeSciencesIntelligence that mergers and acquisitions provide significant industry benefits, promoting innovation and discovery.
“M&A provides an avenue to reinvest in emerging science and to ensure that the pipeline keeps flowing,” noted Chancellor.
When big companies with more capital purchase smaller innovative companies, they establish a symbiotic relationship where the parent company benefits by adding to its portfolio, and the acquired company has the funding to continue innovation.
Saarony explained that innovative biotech companies acquired by larger pharmaceutical practices sometimes do not have to integrate fully into the business. Instead, they can function as a sub-company.
“They allow them to run in a more nimble, innovative way. So, what [the companies] are getting is a well-funded startup, which is great for the ecosystem and everyone. Most importantly, it’s great for patients who hopefully get therapies.”
“The days where pharma may have bought something to shelve it are long gone,” continued Saarony.
Opportunities
As with any industry, mergers and acquisitions in life sciences evolve with the pace of the market and economic climate. Sometimes, these changes result in challenges that limit M&A development, while other times, they present opportunities for growth and further progress.
Oddly enough, challenges securing capital have benefited the more prominent players in the industry who are hoping to acquire smaller companies.
“Curavit focuses a lot on the smaller end of the market, innovative companies, digital therapeutics, and digital health companies,” Morse prefaced. “They have struggled with the capital markets. They’ve dried up at the end of 2022 and certainly into 2023, which hurt innovation.”
The difficulty of securing capital has caused the costs of these companies to go down, presenting an opportunity for more prominent companies to round out their portfolios and fill the pipeline.
“[Curavit] sees that as a huge positive because that additional investment can go into some innovative companies, which is healthy for the entire ecosystem,” Morse continued. “The big players, like the Mercks, Pfizers, and Sumitomos of the world, have the capital to make investments in innovative companies that have worked hard and, in some cases, gotten over the line with the FDA but need market access and more health economic research.”
Another opportunity that is expanding M&As in life sciences is the looming patent expirations approaching. As companies lose market exclusivity, they need to acquire novel assets that can generate the revenue they will inevitably lose upon the emergence of generic therapeutic alternatives. While that may be challenging for companies holding the patent, it lends itself to a more significant number of acquisitions to add to their portfolios.
“Larger companies face patent cliffs of varying sizes, which necessitates refreshing their product portfolios, especially in light of the Inflation Reduction Act,” Chancellor noted.
Challenges
Conversely, securing capital can challenge companies looking to acquire or merge with other players.
Another challenge Morse and Saarony identify is Security and Exchange Commission (SEC) scrutiny. The SEC is a US regulatory agency that enforces security laws, regulates security markets, monitors disclosures, protects investors, oversees investment funds, and promotes good corporate governance practices.
When life sciences companies engage in M&A activities, they must disclose material information about the proposed transaction to their shareholders and the investing public, including details about the terms of the deal, potential risks and benefits, financial implications, and any regulatory approvals required. The SEC reviews these disclosures to ensure they comply with the applicable rules and regulations, such as the Securities Act of 1933 and the Securities Exchange Act of 1934.
The SEC’s role also includes monitoring and ensuring compliance with insider trading regulations during M&A transactions. The SEC investigates and takes action against any potential violations of insider trading laws to maintain the integrity of the securities markets.
Furthermore, the SEC may scrutinize M&A transactions from an antitrust perspective. Alongside other regulatory bodies, such as the Federal Trade Commission (FTC), the SEC evaluates whether proposed mergers or acquisitions in the life sciences industry could substantially lower competition or harm consumers. These reviews help determine whether the transaction should be approved or subject to further examination.
According to Morse and Saarony, the SEC is becoming more scrutinous of mergers and acquisitions, with more criticism on what it’ll approve and a focus on antitrust. These barriers may challenge companies in this space, altering negotiations and potential collaborations.
“FTC will continue to scrutinize deals, although the go-ahead for Amgen–Horizon and likely approval of Pfizer–Seagen bodes well,” Chancellor predicted.
EVALUATING AN ACQUISITION
LifeSciencesIntelligence asked the experts to explain what may make a life sciences company appealing for an acquisition or merger. Understanding these factors can help guide future deals or prompt companies to make changes that improve their appeal.
“In pharma, it’s simple. Does it compliment their pipeline or fill a gap at the end of the day?” posed Saarony.
He adds that the current landscape, especially with service and technology providers and clinical research organizations (CROs), is fragmented and ready for consolidation.
“We’re about the ethical compliant conduct of clinical trials,” explained Sarrony, providing an example of how mergers and acquisitions must align with the company’s overall mission. “I’m not going to get into any services or technologies that, by definition, are the antithesis of that.”
“My important client sets are CROs,” he added. “I’m not going to get into any services or acquire any companies that compete with CROs; it’s too much of a channel cost.”
The examples provided by Saarony are based on his organization’s needs; however, each company’s decision is seen through a different lens, depending on their goals and business models.
“Acquiring companies are often looking for near-term growth drivers, which means late-stage pipeline drugs are in high demand,” added Chancellor. “For earlier-stage drugs, the conversation is often about licensing and partnering, which allows both sides to mitigate the risks associated with R&D.”
For instance, in the two examples mentioned before, the Pfizer–Seagan and Roche–Carmot deals, the companies chose their acquisitions because they added a particular asset aligned with their company goals.
In the Pfizer–Seagan deal, the company hoped to add to its oncology portfolio, making Seagan’s four FDA-approved drugs particularly enticing. In 2022, Seagan’s revenue increased 25%, generating roughly $2 billion, including $1,707 million from total net product sales.
Beyond that, Seagan predicted that 2023 would generate approximately $2.2 billion in revenue, accounting for a 12% year-over-year growth. Additionally, Pfizer estimated that Seagen will generate roughly $10 billion in 2030 and continue to amass income by advancing and expanding its existing oncology portfolio. Both of these projections factored into acquisition choice.
For the Roche–Carmot deal, three obesity assets in late-stage clinical trials present an opportunity in the growing obesity drug landscape.
Beyond looking at the patient improvement lens, which is the primary end goal for all of these organizations, Morse adds that companies are considering whether the assets acquired during a business transaction are a marked improvement — regarding health outcomes and health economics.
“In the current environment, where M&As are typically bolt-on acquisitions rather than large mega-mergers, the most attractive candidates have a narrow therapeutic focus and best-in-class or first-in-class assets,” noted Chancellor.
Beyond determining the actual acquisition and whether it is a good fit, companies must be prepared for the integration of the two entities.
“Getting it right in terms of having bought the right asset is maybe 50% of the story at most,” began Saarony. “It’s ensuring that it functions afterward, that [the acquiring company] doesn’t lose the key people or clients.”
“Day one, all the back-office systems get integrated,” asserted Saarony. Beyond the system integration, the companies switch to the new policies and procedures of the parent company. It takes time to dissolve the old protocols and bring in the new ones, but that is paramount before considering product synergies.
“First, we want to stabilize the house and ensure that we preserve the best of the culture from both companies, the acquired and the acquirer, making sure that there’s clarity around who we are — we’re one company,” said Saarony.
Morse added, “It is important to make the company that’s being acquired feel at home. And part of that is making sure that everything is the same, which takes a while.”
According to AON’s M&A Risk in Review report, approximately 98% of M&A deals teams prioritize talent acquisition, retention, culture, and leadership as moderate-to-significant focus areas.
“A good portion of our revenue gets generated from people. When acquiring a company, we don’t want to lose the people who are generating the revenue. This is a very pragmatic financial view,” said Saarony.
Although companies in the Aon report list employment law and labor relations as the primary workforce concern, acquirers must also consider the company culture and the environment. In descending order, the following factors are regarded as secondary workforce concerns: culture alignment, leadership and talent retention, pension liabilities, and headcount synergies.
“In general, as much as we’re buying products, we’re buying people, and you better learn how to retain them and keep them happy,” added Saarony, revealing that redundant roles will be eliminated. Still, companies should consider how to keep staff happy during the acquisition.
PREDICTIONS
Beyond providing insight into the M&A landscape, the experts also provided predictions for the industry in the coming years. “Wider macro environment suggests that M&A levels should continue to pick up,” predicted Chancellor.
Morse and Saarony echoed the excitement and positivity looking toward the future.
“It’s an exciting time, and we’re bullish on 2024. Look out for a lot of activity that we can’t even probably predict right now,” noted Morse.
“The great thing about our industry is it is resilient. [It’s] going to have the ups and downs of the economy, the political environment, and the social environment,” Gadi added. But “our industry is resilient. Innovation will continue. The focus on driving and then delivering therapies to patients will continue. R&D will thrive.”
As we kick off 2024, we wanted to start the new year with a series of 2024 Health IT predictions. We asked the Healthcare IT Today community to submit their predictions and we received a wide ranging set of responses that we grouped into a number of themes. In fact, we got so many that we had to narrow them down to just the best and most interesting. Check out our community’s predictions below and be sure to add your own thoughts and/or places you disagree with these predictions in the comments and on social media.
All of this year’s 2024 health IT predictions (updated as they’re shared):
And now, check out our community’s Pharma IT and AI predictions.
Archana Hegde, Senior Director, Integrated PV Solutions at IQVIA
The evolution of artificial intelligence (AI) such as generative AI has just begun. The excitement around new tools took hold of all industries in 2023, and the potential is expansive. In the coming year, we will see more AI tools begin to be built into existing workflows, rather than acting as a standalone aid. For the pharmacovigilance space, for example, this automation will begin as a tool for recommendations, suggestions or options for potential safety reports, but it will not fully replace human efforts particularly as there are concerns around data output consistency. It is key for pharmaceutical companies to recognize that efficiency does not override compliance, patient safety or regulatory standards.
There is a growing interest in the integration of safety services with technology, and this will continue into 2024. With subject matter experts providing necessary insights to guide technology, companies will see efficiency, cost savings and overall collaboration.
Though organizations will look to conduct this integration quickly, they must first construct roadmaps for this fusion, as an overall “instantaneous” approach will not be sufficient or feasible. The unification of technology, services and pharmacovigilance expertise in the coming year will further enunciate the industry’s focus on patient safety.
Joel Morse, CEO & Co-Founder at Curavit Clinical Research
1) Digital Therapeutic (DTx) companies will continue to pivot away from prescription models. In 2023, Pear Therapeutics filed for bankruptcy and Akili abandoned the prescription business model. Both DTx companies raised hundreds of millions of dollars by going public in SPAC transactions. While each company successfully gained FDA approvals, the current market acceptance for prescription digital therapeutics is low and improvements will take years. Given this, many DTx companies will pivot away from the prescription model and go straight to consumers next year. They will continue to run clinical trials to confirm their claims and value proposition but will not seek FDA approvals.
2.) Health Economics Outcomes Research (HEOR) will become more common in decentralized clinical trials (DCTs). This year we saw the maturation of Claims and Health Information Exchanges, which enable a cost-effective and straightforward process for researchers to gain access to identified patients’ data. Given the improvements in costs, trial sponsors can now take advantage of these exchanges at scale and leverage the data for both pre-screening and health economic analysis. As DCTs and virtual site acceptance accelerates, a knock-on effect will be that more of these trials will include HEOR analysis.
Jane Reed, Director of Life Sciences at Linguamatics, an IQVIA company
Pharmaceutical developers have always prioritized drug safety. Now, they have new tools such as artificial intelligence (AI) and machine learning (ML) that they can leverage to automatically scour medical literature for information to assist signal evaluation and medical review, or real-world-evidence insights that can lead to drug-safety improvements. Drug developers can use these tools to inform routine information-discovery tasks that would require much more time for humans to execute, including benefits-risk evaluation and safety assessments. Combining different types of NLP (deterministic rules-based NLP, transformer models, LLMs for generative text) enables teams to use the right tool for each task, combining automation with human-in-the-loop review for expert validation.
Riccardo Butta, President of the Americas at Stevanato Group
In 2024, we can expect progress around men’s health, specifically in prostate cancer. Today, the five-year survival rate is nearly 100% thanks in part to the development of Monoclonal Antibodies (MABs) which mimic natural antibodies and recognize and attack specific proteins on cancer cells.
The spotlight won’t just be on science; pharma companies will share the stage. Discussions will focus on the nuanced packaging and delivery requirements for MABs, emphasizing the commitment to safety standards while ensuring the drugs’ effectiveness.
AI/Automation in Pharma and Healthcare
In 2024, the pharmaceutical landscape can expect a continued shift as AI continues to reshape drug development and healthcare practices. Across genomics, proteomics, and patient data, AI algorithms are beginning to decipher vast datasets to discover new drug targets, refine clinical trials, and tailor treatments to individual patients. The application of machine learning and deep learning is enhancing the creation of predictive models, cutting costs, and simplifying the timelines of drug development.
AI’s influence also optimized drug manufacturing processes, enhancing efficiency, and reducing waste. The AI revolution has been and will continue to redefine the pharmaceutical industry in 2024, promising transformative outcomes for patients.
Dave Latshaw, CEO at BioPhy 1. Significant Increase in Big Pharma M&A as Biotech Rebounds
Data-Driven M&A Strategies: In 2024, generative AI is expected to significantly aid in sifting through vast datasets to identify optimal M&A targets in the biotech sector, focusing on companies with innovative pipelines and technologies that align with Big Pharma’s strategic goals.
Streamlining Due Diligence with AI: AI technologies will likely be crucial in conducting efficient and thorough due diligence, examining potential M&A targets in the biotech industry for their scientific innovation, financial stability, and market compatibility.
Enhanced R&D Synergy Identification: By analyzing research portfolios and pipelines, generative AI can identify synergies and complementary assets between companies, guiding decisions on mergers and acquisitions to foster innovation and growth in biotech.
2. Bigger Focus on Pharma Supply Chain Resilience Due to Threats Resulting from Geopolitical Issues
Scenario Modeling for Supply Chain Risks: Generative AI can create complex models that simulate various geopolitical scenarios and their impact on the pharma supply chain, aiding in the development of robust contingency plans.
Predictive Analytics for Supply and Demand: The technology will likely be employed to predict supply and demand dynamics affected by geopolitical changes, enabling more agile and responsive supply chain strategies.
Diversification Strategies: Predictive AI can assist in identifying alternative suppliers and logistic routes, helping pharma companies diversify their supply chain to reduce reliance on geopolitically sensitive regions, thus enhancing overall resilience.
3. Streamlining Regulatory Compliance with AI
Automated Compliance Monitoring: In 2024, AI is predicted to automate the monitoring of regulatory compliance in drug development, efficiently tracking changes in global regulatory requirements and ensuring adherence to these evolving standards.
Predictive Analytics for Regulatory Approval: AI’s predictive analytics capabilities could forecast regulatory approval outcomes based on historical data, helping companies to strategize and address potential regulatory hurdles in advance.
Enhanced Documentation and Reporting: AI tools are expected to streamline the documentation and reporting processes in regulatory affairs, using natural language processing to generate and organize required documents more accurately and swiftly.
AI-Enabled Regulatory Intelligence: In 2024, AI is anticipated to enhance regulatory intelligence by continuously scanning and interpreting global regulatory landscapes, aiding pharmaceutical companies in effectively navigating different regulatory environments.
Facilitating Stakeholder Engagement: AI tools might be employed to facilitate better engagement with regulatory stakeholders, by analyzing feedback and guiding pharmaceutical companies in addressing regulatory concerns more effectively and collaboratively.
Updesh Dosanjh, Practice Leader for Pharmacovigilance Technology Solutions at IQVIA
In 2024, the traditional pain points of the pharmacovigilance (PV) space will not disappear. Case volumes will continue to grow while the number of individuals working in the field will not follow suit. The PV model is broken, and in 2024, companies will need to assess how automation can fix operations. While this automation is necessary, there is hesitation to implement technologies and tools such as generative artificial intelligence (AI) and machine learning (ML). Before incorporating advanced automation, organizations must take a holistic look at their processes. Adding automation to an inadequate process will help mitigate issues in the short term but will be detrimental for long-term operations. The PV space is resistant to change, especially because validating new systems can take months. However, organizations need to proactively make a shift, or this change will be forced upon them.
In the upcoming year, we will see the expansion of new, more complex markets and updated requirements from regulators. The balance between monitoring for these adjustments and maintaining the growing volume of cases will be tenuous. Without fixing the current, broken PV models, the continuous cycle of more complexity in the market, which then pushes organizations to incorporate automation into insufficient processes, will massively hinder PV operations. This will become more evident in the upcoming year, and organizations will be forced to reimagine their models.
Pouria Sanae, CEO at ixlayer
In 2024 we can expect care teams to get bigger, broader, and more collaborative as new digital tools and care strategies combine to shift the status quo. Convenience, cost, and consumerism remain top-of-mind going into the New Year, and more healthcare stakeholders are considering offering at-home tests to close gaps in care and advance better health.
For example, pharma companies are now starting to engage in at-home diagnostic testing initiatives, including telehealth consults to review results – a task traditionally assigned to primary care and specialists. The trend is driven by a growing focus on health equity and proactive, personalized care. Sending tests to patients’ homes helps overcome SDOH barriers that may prevent patients from getting to a lab for testing. This will lead to more comprehensive screenings, which in turn will result in earlier diagnosis and treatment of chronic disease. For pharma companies, that means a significant number of patients who could benefit from currently available therapies may soon be getting the treatments they need to stay healthy.
Michelle Gyzen, Senior Director, Regulatory Affairs and Drug Development Solutio at IQVIA
The desire for rapid adoption of intelligent automation technology will be widespread in 2024. While tools like artificial intelligence (AI) show a lot of promise for the pharmaceutical regulatory industry, many are not quite ready for all the challenges that will follow. There are considerable risks to adoption that may have deep compliance implications. Human efforts are the greatest asset in the journey to automation in terms of compliance and validation, and organizations will see this firsthand in the upcoming year.
As new systems and automated technologies are built, global health authorities will need to respond accordingly. In the next few years, we will see greater collaboration and consolidation with how health authorities will accept submissions. There will be a big push for component content management, and possibly the reinvention of the electronic common technical document (eCTD). Though it may not happen in 2024, the industry will take some strides to eventually see end-to-end automation for eCTD submissions. The most exciting aspect is the potential of the combination of AI, machine learning and large language models to help decipher and manage health authority communications. By leveraging an organization’s intelligence and existing information, organizations will be able to efficiently respond to health authority queries with the assistance of AI.
The regulatory industry is typically hesitant to embrace innovative technologies. However, in the past year, there was a new understanding and appreciation for what can be achieved and optimized. This will push organizations to look towards the phased implementation of automated tools for the regulatory field. In the same vein, we expect organizations to take a more thoughtful approach, really taking time for change management, retraining and repurposing staff as automation enhances their work.
Jason Rose, CEO at Adhere Health
2024 will spark transformational change across the pharmaceutical industry. CVS’s proposed drug pricing formula is likely to compel other major retail pharmacies to move to more transparent, lower-cost pricing models. While this shift may ultimately lead to lower costs for consumers, it could also create additional problems for certain rural and urban areas with “pharmacy deserts” as independent pharmacies may not have the scale and efficiency to compete.
This pharmacy desert challenge is an important social determinant of health (SDOH) barrier that leads to reduced health equity for vulnerable, higher-risk consumers. Independent pharmacies have struggled for years to stay afloat as they deal with issues such as DIR (direct and indirect remuneration) fees. It is important to ensure our most vulnerable people are getting the proper care and health equity.
Simon Johns, Director, Medical Information and Marketed Product Safety at IQVIA
The continuously growing volume of Medical Information case inquiries will not cease in 2024, especially as it is effectively the only inbound communication channel remaining for pharmaceutical companies. Artificial intelligence (AI) will be relied on to help manage the growing case volume. Although AI is not a novel concept within the pharmaceutical industry, the introduction of new systems and tools – like generative AI – will push companies to revisit their current applications to automate traditionally manual tasks.
In 2024, the industry, specifically within the Medical Information area, will see shifts to multi or even omni channel models to ensure that healthcare professionals and patients have available means of communication with pharmaceutical companies when necessary. AI chatbots will first be applied to this area in the form of warm transfers – if a call center is experiencing a surge in calls and all human agents are occupied, AI agents will emerge as a backup. These chatbots would then be able to transfer the inquiry to a human agent when available or needed. Fully automated processes will be phased in. Against some beliefs that this process will replace agents, AI will be a tool for agent assistance and faster response.
Maintaining compliance is a priority for pharmaceutical organizations, and while the gradual integration of AI processes may seem like a large endeavor, organizations will begin to see the benefits in the upcoming year.
Ian Chan, CEO and Co-founder at Abpro
The global supply chain issues and continued difficulties securing funding amid economic uncertainty caused challenges for many life sciences companies this year. In 2024, I believe we’ll see an uptick in innovation across the industry, especially as AI capabilities continue to progress and become more and more ingrained in a myriad of applications – from expedited drug development to accurately identifying diseases. I anticipate that smaller biotech companies will consider multiple avenues for securing funding, including through SPAC deals similar to the one that we at Abpro announced this year. The top priority for biotech in 2024 will be getting potentially life-altering therapeutics into the hands of the patients who need them more quickly and efficiently.
Dr. Kate Sasser, Chief Scientific Officer at Tempus
AI is accelerating drug development and fueling enrollment in clinical trials: AI-enabled diagnostics and AI-empowered clinical trials will expand and start to drive greater impact in the clinic and in drug development. As drug development gets more precise, finding very specific patient profiles for clinical trials or therapy, becomes much harder. With larger, interconnected data sets in the healthcare systems, AI will be able to identify those needle-in-a-haystack patients, and match them to the appropriate clinical trials or therapies.
Manu Garg, Vice President, Head of Healthcare Consulting at Definitive Healthcare
AI adoption will be crucial for biopharma and medical device companies in 2024. While 42% of life science leaders state lack of skilled talent as a roadblock to AI adoption in their institutions, we will see more life science leaders collaborating with large tech companies to build and pilot programs that meet organizational needs. Collaborating with experts from tech companies will empower life science businesses to embrace the technology and negate major fears around security, quality and ethics of AI implementation.
Michel Denarie, Senior Principal, RADDS at IQVIA
In the coming year, clinical trial sponsors will become even more focused on implementing diversity plans and this will continue to push for major shifts across the industry. In fact, within the United States, guidance has been introduced for the creation of diversity plans in clinical trials to push further diversity and inclusion. This is a critical step for drug development as patients must be representative of the population, but it is key to note that it must be done cautiously to be compliant with the expectations of health authorities.
Project optimizations from the FDA, specifically Project Optimus within oncology, is a recent trend that will expand to other therapeutic areas in the coming year. Rather than testing only the maximum efficacy, organizations have been pushed to find the therapeutically optimal drug dose. This dose optimization could soon be a de facto requirement, elongating the trial process and increasing overall costs – beyond oncology.
In terms of indication prioritization, organizations will begin to integrate natural language processing and artificial intelligence for optimization and efficiency. This automation will help reduce the manual time spent on data analysis, allowing senior team members to focus more on operations that require a high level of human expertise. This integration will happen slowly, but steady, as automated technologies must be validated for accuracy.
Angie Franks, Chief Executive Officer at Kalderos
There will be continued conversations in 2024 around whether patients are benefiting from drug discount programs, such as 340B and MDRP (Medicaid Drug Rebate Program). And the future of technology in this space will get a lot of attention. We need to explore ways to simplify what has become a complex system to enable greater efficiency and drive down costs. Finally, drug discount stakeholders need to stop being so adversarial and start working together by leveraging tech to streamline processes, enable data sharing, and increase transparency, all of which are critical to building trust. Let’s all focus on how the rebate programs can benefit patients who need drugs at affordable prices. The fighting has to stop if we want to improve healthcare. Fortunately, I think the willingness is there.
Experts anticipate the new year will prove to be an impactful one for data and technology in R&D and clinical trials as companies seek to leverage big data in practical ways, simplify end-to-end data flow for sites, build single platforms for managing data and work together to drive the AI revolution forward. The following are some insights for 2024 from experts at Lokavant and Veeva Systems.Read More
Decentralized trial (DCT) methods will continue to evolve in 2024 as a group effort led by the Tufts Center for the Study of Drug Development (CSDD) to gather/utilize DCT data for informing future protocol designs aims to deliver its first dataset in the first quarter. By the end of 2024, decentralization will have established itself as the new gold standard for trials, experts predict. Read More
With this year’s fully virtual MAGI@home conference delivering high-energy insights and receiving a strong reception from attendees, 2024’s in-person MAGI conference in New Orleans on April 14-17 is sure to generate more of the same. The following is select coverage from the WCG Talks Trials podcast, which discussed MAGI’s success over the years.Read More
As the oncology landscape evolves, evaluating trends and advancements in diagnosis and treatment may inform predictions for the coming year.
– Over the past decade, advancements in the oncology landscape have significantly changed the diagnostic pathway and treatment pipeline. As scientific discoveries inform product development and care strategies, experts predict that the industry will continue to evolve, and prioritizing early diagnosis and treatment.
LifeSciencesIntelligence sat down with Candice Del Rio, MS, BSN, RN, Director of Clinical Operations at Curavit, and Julie Ozier, Senior Vice President of IRB Review at Advarra, to discuss the current oncology landscape and predictions for the coming year.
ADVANCEMENTS IN ONCOLOGY
Throughout the discussion, both women highlighted recent advancements in the oncology landscape that may result in transformative differences for patients and providers. Changes in the regulatory environment, new risk assessment protocols and tools, and therapeutic discoveries are critical components that have guided the evolution of oncology.
Regulation
One component is the regulatory aspect, which includes clinical trial protocols and participant guidance. As new treatments come out and evaluations of study protocols identify strategies for improving therapeutic outcomes, regulatory bodies, including the United States Food and Drug Administration (FDA), have adjusted their guidance to reflect discoveries.
For example, Del Rio noted, “The FDA’s recent update on including older adults in oncology is important. It’s more inclusive and focuses on people who are likely to receive treatment.”
In 2022, the FDA issued a final guidance, “Inclusion of Older Adults in Clinical Trials,” encouraging researchers to include older adults in cancer clinical trials. Supporting President Biden’s cancer moonshot effort, these recommendations urge involvement in early clinical trials and provide recommendations for trial design, recruitment, information collection, and reporting for older populations.
Risk Assessments
Del Rio also notes that critical technological evolutions have advanced the understanding of who is more likely to have a malignancy, allowing providers and researchers to assess cancer risk more accurately.
“For instance, proteomics is super smart. It focuses on how protein expressions will reflect a physiological state. It’s very accurate and precise,” she explained. “Providers can use it to target or determine an early intervention or even early treatment, which is impactful in terms of how and who gets treated for oncology stays.”
Multi-omics profiling — which includes proteomics, measurements focused on proteins and their expression; metabolomics, focused on metabolites; and transcriptomics, focused on transcriptomes — has been explored for diagnostics and gathering health insight data.
Beyond proteomics, developing new target therapies that leverage the body’s immune system and other biological tools to fight cancer has marked a significant advancement in oncology.
Ozier emphasized the , including chimeric antigen receptor (CAR) T-cell therapy and mRNA therapeutics, coming down the pipeline.
Since the first FDA approval of CAR T-cell therapy in 2017 for pediatric and young adult patients with acute lymphocytic leukemia, CAR T-cell therapy has been implemented for multiple indications. Despite recent FDA investigations into the safety and risks associated with CAR-T, many medical professionals and scientists maintain that the benefits of this targeted therapy outweigh the risks.
Besides cell therapy, Ozier included that gene editing and genetic manipulation technologies, like CRISPR, are bringing new treatments to market.
SCREENING AND DIAGNOSIS
Although these advancements have improved patient outcomes and provided additional tools in the oncology landscape, patient survival hinges on diagnostics and treatment access. Focusing on diagnostic tools and screenings, Del Rio explained, “Screening typically is a standardized process. It can be for healthy patients; it can be for anyone more at risk.”
While the screening rate changes depending on patient risk and life stages, the general premise is the same.
On the other hand, diagnostics are used when an issue is suspected, or abnormalities are detected during a screening.
“It’s interesting how the same tool can be used for screening and diagnostics. Mammography is a good example.”
Prioritizing Screening and Diagnostics
While developing new technologies is critical and impactful in the oncology space, applying, leveraging, and effectively using these tools is what makes a difference in patient outcomes. Leveraging these technologies for early detection, diagnosis, and treatment is vital to making these tools valuable.
“Part of that process is the traditional approach of having people come into clinics, running the usual diagnostic tests. But part of it is understanding that true early prevention and detection involves bringing those technologies to the patient,” noted Del Rio. “People are trying to move in the direction of making it more realistic, more user-friendly, and reducing the pain point as part of making tools for real-life use.”
The shift toward more accessible and favorable screening and diagnostic tools may support earlier disease detection.
“The hope [with early detection] is that there won’t be anything metastasized. The earlier [a provider] can detect something, it might be in place, as opposed to metastasizing and then getting out of control and being much worse,” Ozier told LifeSciencesIntelligence.
Despite the widespread understanding that early detection and early screenings are indicators of patient outcomes and survival, a NORC study published in 2022 determined that only 14% of cancer in the US are detected through screenings, pointing to a discrepancy between the understanding of screening importance and the application.
Part of the discrepancy can be accounted for by the limitations in screening. There are only screening tools and options available for some cancers, and those screenings may be done at varying ages or stages of life.
“Some of the screening can be viewed as invasive,” added Ozier, implying that it may deter patients from screenings.
Structural Limitations
However, other controllable factors have also contributed to this gap. For example, Del Rio notes, “The latest US census report from 2022 noted that about 8% of Americans don’t have health insurance. That’s the minority, but it’s a contributing factor.”
Most patients cannot afford to get screened as recommended without health insurance. Additionally, patients without insurance who are experiencing symptoms may put off seeing a physician due to financial restraints.
Beyond that, Del Rio explained, “There’s an element of control by insurance companies. How early can someone get in to see an appointment, and is that provider covered under someone’s insurance? And anyone who knows someone or who has experienced cancer themselves would know that it can be a very long, expensive process.”
Social Limitations
In addition to structural barriers that limit access to screenings, social factors contribute to low screening rates. For example, some patients are scared to get screened. Del Rio points out that, for some patients, knowledge can be scary, so getting to screenings may be anxiety-inducing for some patients.
Moreover, a health literacy gap may be contributing to low screening rates. Some patients may not know or understand the importance of screenings, where to access them, or what to do with that information once they have it.
Improving Access Through Data Analytics
The oncology landscape may be able to incorporate data analytics and technologies to streamline and shorten the diagnostic pathway.
“There’s a lot of data sharing, especially through NIH’s dbGaP, their whole project on data sharing, and wanting institutions to share data across health exchanges like electronic medical records sharing,” Ozier revealed. “The regions are pooling together their data. We’re at the beginning of this sharing, but that will lead to faster diagnosis, better screening, and better treatments overall.”
FUTURE OUTLOOKS
Del Rio and Ozier provided LifeSciencesIntelligence with some predictions for the oncology landscape in the coming year. They emphasized improving the diagnostic pathway and continuing to build on existing technology.
“Bringing options to patients where they are, making it easier, and making it less painful, literally and figuratively [will be a priority],” said Del Rio.
Part of that means making it easier to access treatment and clinical trials. “Decentralization, bringing things to the participants or the patients, is important,” said Ozier.
Beyond access, technological advancements that provide targeted therapeutics will be prioritized.
“With all of the technology and with the proteomics, that it’ll be more targeted therapy to certain groups, [depending on] who responds better to what,” Ozier said.
Decentralized clinical trials (DCTs) are gaining increasing interest as they have the potential to make clinical trial operations quicker, more efficient and more accessible to patients. Check out five DCT organizations that have raised big venture capital investments in the last few years.
The world’s population is aging. In the United States alone, the number of people aged 50 and older is expected to increase by more than 60% by 2050.1 And of that older population, the number with at least one chronic disease is expected to nearly double over the same period. The increasing pervasiveness of chronic disease in the coming decades not only has the potential to threaten the lives and well-being of many more Americans, but it will also put additional pressure on an already burdened healthcare system, stretching exorbitant costs even further.
In the face of this wave of aging patients and burgeoning instances of chronic disease, digital therapeutics (DTx) have the opportunity to serve as a lifeline. The research has suggested that DTx products can save lives and improve outcomes for people living with chronic disease; in fact, a 2021 study2 showed a 52% lower risk for all-cause 30-day readmissions among patients with acute myocardial infarction (AMI), a condition that not only threatens people’s lives but also burdens an overtaxed healthcare system. Another study found DTx innovations to be highly effective in improving glycemic control and weight loss in adults with Type 2 diabetes, thereby improving their long-term health while reducing reliance on traditional drugs.3
Over the last decade, DTx therapies have also played a significant role in the effective management of a variety of mental health issues. Many digital therapies have offered solutions to substance abuse, sleep disorders, depression, ADHD, and more. According to the World Health Organization, nearly a billion people worldwide live with a mental health disorder, yet three-quarters of these individuals receive no treatment, either because of a lack of access to care or the stigma surrounding their condition.4 DTx therapies have already made headway in closing this gap by providing more options, as well as convenient and discreet access to care for those in need.
Despite DTx effectiveness in cost-effectively treating chronic conditions and mental health disorders, some could argue that healthcare professionals (HCPs) have been slow to prescribe or recommend them to patients. The reasons for this are complex and multifaceted, but they begin with the industry’s chronic difficulty adapting to change.
“When Medicare was created in 1965, the thought was that healthcare would always be delivered at the doctor’s office,” said Andy Molnar, CEO of Digital Therapeutics Alliance, a trade organization focused on the needs of the DTx industry. “It took until the early 2000s before there was even a pharmacy benefit for Medicare, so it’s not really the most progressive program.”
The lack of widespread knowledge and understanding about DTx products among clinicians, as well as complications with prescribing these therapies, various administrative challenges, and insufficient insurance coverage have all added to the ongoing obstacle of getting these treatments into the hands of those who they can help, despite their proven efficacy.
Moreover, the entire process of development has proven to be fraught with challenges as well. For example, DTx companies often struggle to conduct clinical trials for their products because of the lack of principal investigators who have enough exposure to such products. And further along in the development cycle, once DTx products have proven to be effective in clinical trials, they face the daunting challenges of FDA approval and payer reimbursement, processes that were originally designed for more traditional therapies.
The fate of Pear Therapeutics, which introduced the first prescription digital therapeutic (PDT) to treat substance use disorder and insomnia five years ago, offers a practical illustration of this challenging marketplace. Despite its groundbreaking innovation, as well as its willingness to go above and beyond the regulatory guidelines necessary to prove the efficacy of its product, Pear struggled to get clinicians and patients to adopt it and payers to reimburse it for those who did. The company went bankrupt in late 2023. According to Pear’s own research, the adoption rate for their product was just 40% among the minority of payers who had familiarity with DTx products.
Safety and efficacy may not be enough
Clearly, producing safe and effective DTx products that improve outcomes for patients may not suffice. The road to viability is longer and more daunting. One solution can be found in the health economic value of DTx products. The more that companies can prove both efficacy and value, the better opportunities they will ultimately have at improving market access, payer coverage, and clinician and patient adoption.
As healthcare costs continue to rise, payers are concerned with health outcomes and cost-effectiveness; this is particularly the cause for less-understood digital therapeutics. It’s critical to capture evidence of the value of these innovations both as it pertains to individual patients in certain therapeutic areas as well as their impact on the broader population.
“Targeted clinical trial, economic, and real-world data will drive adoption of DTx products,” Molnar explained. “Capturing the right data that proves to all stakeholders—government, commercial insurers, medical directors, providers, and patients—to adopt these products, however, is complex. It is even more daunting for DTx startups that may not have the same resources as pharmaceutical companies.”
To be successful, DTx companies must find efficient ways to capture health economics data from day one—a guideline that MedRhythms, a rapidly growing DTx company that produces neurotherapeutics, has followed.
“A cornerstone of our mission is that our products must be accessible to patients. One way we do that is through furthering our evidence development,” said Owen McCarthy, president and co-founder of MedRhythms. “We need to speak the same language as payers in order to gain traction for a new prescription-only product just as much as we need to demonstrate efficacy to providers.”
An alternative direct-to-patient model
After the demise of Pear, other leading DTx companies began to rethink their commercialization models, even bypassing the need for a doctor’s note. While these products no longer require a prescription or FDA approval, they do require the same clinical trial rigor. Companies like Akili Therapeutics5 have opted for this route to ensure broader access to their products while the regulatory infrastructure around reimbursement is established. While the direct-to-consumer model reduces the reliance on payers, it still requires proof of economic value for patients to try these novel digital therapies. In fact, the bar for demonstrating higher health economic outcomes might be even higher for over-the-counter solutions to overcome any fear or distrust inherent to something unfamiliar.
Whether they choose the traditional or direct-to-consumer commercial model, DTx companies must be able to fully harness and deploy data and information that can prove their value. Without this information, these innovative treatment alternatives could struggle to succeed, regardless of how effective they might be.
References
1. Ansah JP, Chiu CT. Projecting the chronic disease burden among the adult population in the United States using a multi-state population model. Front Public Health. 2023 Jan 13;10:1082183. doi: 10.3389/fpubh.2022.1082183. PMID: 36711415; PMCID: PMC9881650.
In a new episode of the pharmaphorum podcast, host Nicole Raleigh welcomes Joel Morse, CEO and co-founder of Curavit Clinical Research, and Andy Molnar, CEO of the Digital Therapeutics Alliance (DTA), for a discussion on why it is that digital therapeutics (DTx) are effective and safe, but not being prescribed.
A virtual contract research organisation (vCRO), 2020-founded Curavit specialises in decentralised clinical trials (DCTs) for DTx, while the DTA works to enable expanded access to high-quality, evidence-based DTx for patients, clinicians, and payors in order to improve clinical and health economic outcomes and provide the digital health ecosystem with the necessary tools to define, evaluate, and utilise DTx products.
Doctors once trying to use fax machines to provide one of the most advanced technologies in the industry, Molnar explains the passion that propels him in his work, and Morse describes Curavit’s latest Health Economics and Outcomes Research (HEOR) practice for pharmaceutical clinical trials, collecting endpoint data to prove medical value, capturing insurance claims and medical record data, the latter quantifying the spending necessary, as undertaken in a recent MedRhythms trial.
Getting the data together to prove to all key stakeholders to adopt these products is quite complex, Molnar says. To provide a new technology, it has to be believable to the broad population and the providers that give care. Indeed, Morse states there is a lack of understanding in the healthcare ecosystem when it comes to DTx.
A lot of the time, the biggest challenge is finding a principal investigator (PI) that has exposure to Software as a Medical Device, for instance. There is a material effort to educate the ecosystem on providing a new genre of healthcare, therefore, and the medical community in the US is a learning community. The conversation also considers the European scenario in passing.
It’s not good enough to just show efficacy, economic value needs to be shown, in DTx and across the board.
You can listen to episode 105a of the pharmaphorum podcast in the player below, download the episode to your computer, or find it – and subscribe to the rest of the series in iTunes, Spotify, acast, Stitcher, and Podbean.
The CenterWatch Monthly provides clinical research professionals with valuable and exclusive content on clinical trial news, trends, analyses and regulatory guidance, as well as expert insights not found anywhere else. The following commentary on DE&I by Rachel Rangel, clinical trial specialist at Curavit Clinical Research, is an excerpt from the December issue’s Year in Review feature.
In 2023, the life sciences industry reupped its commitment to improving diversity, equity and representation in clinical trials. Sponsors have historically failed to achieve adequate representation of minority groups within their clinical trials, but thanks to new regulatory legislation issued by the FDA that requires sponsors of certain clinical trials to submit diversity action plans, report demographic data for participants and actively recruit from underrepresented populations, top pharmaceutical companies are now prioritizing DE&I across their trial portfolios.
For instance, in March 2023, Bristol Myers Squibb announced a multimillion-dollar investment in its global inclusion and diversity goals, including a focus on increasing clinical trial diversity. The company claims that nearly 60 percent of its clinical trial sites are now located in racially and ethnically diverse areas of the country. By embedding more clinical trial sites in diverse communities, BMS is helping enroll clinical trial participants that are more reflective of the broader patient populations they aim to serve and better aligned with the epidemiology of the diseases studied.
While the industry is moving in the right direction, racial and ethnic minorities still only account for 2 percent to 16 percent of trial participants despite comprising 39 percent of the U.S. population. One of the biggest obstacles is patient recruitment and retention from historically underrepresented populations. To overcome these challenges, sponsors like MedRhythms are starting to collaborate with partners that specialize in diverse patient recruitment to carefully plan and execute recruitment and retention strategies that reduce some of the traditional barriers to study participation and are more conducive to reaching a broader demographic.
Actionable solutions that are gaining popularity in diverse participant recruitment include:
Implementing modern research models, such as decentralized clinical trials that use virtual sites to meet participants where they are
Engaging with diverse communities through partnerships with community organizations, leaders and medical providers
Fostering diversity in research teams to better understand and empathize with participants from diverse communities
Monitoring diversity milestones in real time to expeditiously rectify any gaps in representation
Addressing cultural linguistic barriers by translating study materials into different languages, using culturally appropriate messaging and providing interpretation services as needed
Swing Therapeutics engaged Curavit Clinical Research to act as a virtual site in a pivotal trial of an investigational digital therapeutic (DTx) for fibromyalgia. Curavit’s clinical operations team recruited, screened, consented, and enrolled participants from across the United States in Swing’s PROSPER-FM randomized clinical trial, and subsequently managed the enrolled participants throughout the 12-week study. By leveraging its virtual site, Curavit was able to eliminate physical and geographic barriers to trial participation, scale quickly, and catalyze patient enrollment.
Curavit’s virtual site randomized 10 times more study subjects than traditional sites that started at the same time. More importantly, Curavit’s virtual site achieved the highest level for study subjects’ adherence to protocol.
Swing Therapeutics designed the original protocol for their Prospective Study to Evaluate a Digital Regimen for Fibromyalgia Management (PROSPER-FM) to fully enable enrolled study subjects to participate from home. The “participate from home” protocol design was meant to improve the study participant experience. The protocol was then adjusted to leverage Curavit’s virtual site for cloud-based screening, consent, and enrollment. At the time, Mike Rosenbluth, PhD, Chief Executive Officer at Swing noted: “Curavit’s virtual services model enables us to efficiently recruit participants representative of the entire patient population.”
Curavit’s virtual site supports diverse patient recruitment and removes geographic boundaries to participation without the expense of physical infrastructure. This increases diversity, patient-centricity, and the likelihood that participants will stick with the trial for the duration.
The type or format of an ePRO also matters as the preference may depend on the participant’s academic background. A study in 2020 showed that there was variability in preference for mobile-based versus website-based methods of ePROs amongst Black and white populations of those with cancer. A small number of Black participants preferred paper methods as they felt there was more time to think about the question, while some found it difficult to understand the paper symptom summary report.
Natalia Husby, solutions manager at CRO Curavit, explains that academic education may play a role in the difficulties experienced with interpreting the summary report. “This finding also highlights the importance of creating study materials that are accessible to people of varied academic backgrounds,” she adds.
When developing and tailoring questions for ePROs, sponsors and vendors should interact with patient communities to understand their experiences. “If it’s not relevant or salient to them, it’s going to be more difficult to recruit and retain,” Husby says. Indeed, improvement in quality of life could mean completely different things across various populations and regions, Mowlem adds.
If sponsors or vendors do not combine their ePROs with user experience, the technical brilliance of a product will not matter. Daniels explains that to improve the understanding of participant diversity, it is important to include patients in the protocol writing or run simulation studies to see if certain populations struggle with some of the questions in the ePRO. “If you can have technology that can adapt to different communities, that is where the culture and the product come together,” she says.
Looking beyond race and ethnicity
Decentralisation and all its methodologies have many features that could improve diversity in clinical trials, but now it is time to show the evidence for it, Mowlem says. Indeed, the data analysis shows that globally, only 27% of DCTs report data on race and ethnicity. “If we don’t report it, we can’t show that we’re improving diversity,” she adds.
The situation is better in the US, with 45% of US-based DCTs reporting diversity data. Yet, Mowlem says this is still quite low. The higher reporting proportion in the US compared to global DCTs may be attributed to the FDA’s effort to increase diversity. However, other regions are not at the same level as the US agency. While the European Medicines Agency (EMA) has a recommendations paper on DCTs,
December is here; the end of 2023 fast approaches. For those operating in the life sciences sector, it’s all too clear that the time has come for 2024 industry predictions.
In a first instalment, we hear from Curavit Clinical Research. Last year, co-founder and chief medical officer Dr Pam Diamond predicted that 2023 would herald the FDA becoming more directive and collaborative on guidelines for decentralised clinical trials (DCTs), that more clinical trials services would become remote (beyond just patient monitoring), that AI innovation would expand its application to enhance patient experience, and that digital therapeutics (DTx) companies would focus on the difficult last mile to commercialisation…
This year, Joel Morse, Curavit’s CEO and founder, and Rachel Rangel, clinical trial specialist, share their predictions for the future focus of digital therapeutics and Health Economics Outcomes Research (HEOR), as well as tunnelling down into the ins and outs of effective DE&I in clinical trials.
DTx: The case for going straight to consumers
Joel Morse thinks that digital therapeutics companies will continue to pivot away from prescription models.
In 2023, Pear Therapeutics filed for bankruptcy and Akili abandoned the prescription business model. Both DTx companies raised hundreds of millions of dollars by going public in SPAC transactions. While each company successfully gained FDA approvals, says Morse, the current market acceptance for prescription digital therapeutics is low and improvements will take years.
Given this, he believes many DTx companies will pivot away from the prescription model and go straight to consumers next year, while continuing to run clinical trials to confirm their claims and value proposition, but not seeking FDA approvals.
Leveraging data for pre-screening and health economic analysis
As pertains to HEOR, Morse thinks it will become more common in DCTs.
This year saw the maturation of Claims and Health Information Exchanges, which enable a cost-effective and straightforward process for researchers to gain access to identified patients’ data. Given the improvements in costs, Morse says, trial sponsors can now take advantage of these exchanges at scale and leverage the data for both pre-screening and health economic analysis.
As DCTs and virtual site acceptance accelerates, a knock-on effect will be that more of these trials will include HEOR analysis, Morse predicts.
Diversity, equity, and representation in clinical trials
Rachel Rangel, meanwhile, notes that last year the industry re-committed to improving diversity, equity, and representation in clinical trials. Thanks to new regulatory legislation issued by the FDA that requires sponsors of certain clinical trials to submit diversity action plans, report demographic data for participants, and actively recruit from underrepresented populations, top pharmaceutical companies are now prioritising DE&I across their trial portfolios.
For instance, in March 2023, Bristol Myers Squibb announced a multimillion dollar investment in its global inclusion and diversity goals, including a focus on increasing clinical trial diversity. The company claims that nearly 60% of its clinical trial sites are now located in racially and ethnically diverse areas of the country.
While the industry is moving in the right direction, though, racial and ethnic minorities still only account for 2% to 16% of clinical trial participants, while they comprise 39% of the US population.
One of the biggest obstacles is patient recruitment and retention from historically underrepresented populations, says Rangel. That’s why sponsors like MedRhythms are starting to collaborate with partners that specialise in diverse patient recruitment to carefully plan and execute new strategies that reduce some of the traditional barriers to study participation and are more conducive to reaching a broader demographic.
Actionable solutions that will flourish in 2024, predicts Rangel, include:
modern research models, such as decentralised clinical trials that use virtual sites to meet participants where they are;
partnerships with community organisations, leaders and medical providers;
diverse research teams who can better understand participants from these communities;
real-time monitoring to expeditiously rectify any gaps in representation early; &
a focus on cultural linguistic barriers, by translating study materials into different languages, using culturally appropriate messaging, and providing interpretation services as needed.
Looking forwards
Be sure to keep an eye out for further 2024 predictions instalments. In the meantime, if you missed the pharmaphorum Frontiers Health 2023 wrap-up podcast, be sure to tune in below for insights on: how digital health and digital therapeutics are shifting the paradigm of care sites; some lessons and discussions from the DTx Global Policy Summit; the current investment landscape; and a broad discussion on AI
You can listen to episode 106 of the pharmaphorum podcast in the player below, download the episode to your computer, or find it – and subscribe to the rest of the series – in iTunes, Spotify, acast, Stitcher, and Podbean.
About the contributors
Joel Morse is founder and CEO of Curavit. He is an experienced operational CEO who has founded, built, and sold large global businesses in healthcare and life sciences. Previously, he founded C3i, a Business Process Outsourcing (BPO) healthcare provider. Morse has a BSc in Mechanical Engineering from Tufts, and an MBA from Columbia.
An audiologist by trade, Rachel Rangel has over 10 years of experience as a medical provider. She has served patients across the US — from rural towns to major cities, in small private practices, children’s rehabilitation hospitals, and large medical systems. As the head of Curavit’s Diversity, Equity, & Inclusion initiative, Rangel is working to make clinical trials a more welcoming and inclusive space to those from traditionally underserved and marginalised communities.
Apps, VR and more could play an increasingly vital role in the wider goals of creating value-based treatments — if the industry can get payers to sign on.
Pharma-created therapeutics have developed beyond pills from a doctor’s office to include apps, virtual reality and video games for anxiety, heart failure, diabetes and more. These prescription software programs, known as digital therapeutics, comprise a growing global market that could hit $13 billion by 2026. This projected growth is being spurred by the numerous advantages of using a personalized and low-risk approach that doesn’t require as many healthcare interventions amid an acute shortage of providers.
So why aren’t more doctors prescribing them?
Some may hesitate to embrace an unfamiliar option or may be stymied by the lack of infrastructure to support prescriptions. But experts say the biggest issue is money.
“Reimbursement is the biggest barrier that we’re facing right now,” said Jessica Hauflaire, COO of the Digital Therapeutics Alliance. Medicare and most commercial insurance companies won’t cover most digital therapeutics, even for FDA-regulated prescription technology, validated to ensure it delivers on its medical claims.
Pharma joins the digital fray
Digital therapeutics companies are now looking to change that by making a financial case to payers, proving the technologies are worth the investment. To that end, Curavit, a virtual CRO, is tracking digital therapeutic interventions and outcomes in clinical trials using Health Economics Outcomes Research. MedRhythms, a company focused on creating neurotherapeutics, is working with Curavit to gather information in a trial for its digital therapeutic MR-001, which aims to help patients regain walking ability following a stroke.
“With the low risk and availability and scalability of digital therapeutic products, I see it becoming the first course of treatment.”
Jessica Hauflaire
COO, Digital Therapeutics Alliance
Data collection will examine whether people stick with the treatment, which uses rhythmic cues to help normalize physical movements, how long treatment effects last, and its potential economic value. Ultimately, Owen McCarthy, president and co-founder of MedRhythms said this information could help prompt changes to the field.
“Three changes that would impact broad access for digital therapeutics: creating clear reimbursement pathways, integrating education about digital therapeutics into medical school curriculum, and continued work on improving workflows for prescribing/dispensing of digital therapeutic products,” McCarthy said.
Pharma’s approach to digital therapeutics
While payers hesitate to embrace digital therapeutics, many pharma companies already see their value.
“We’re working with a lot of big pharmaceutical companies that are partnered with a digital therapeutic company and I think it’s a win, win,” said Joel Morse, CEO and co-founder of Curavit. “The pharmaceutical companies have resources, and they invest in a tremendous amount of R&D. The digital therapeutics companies have a tremendous amount of innovation, and a lot to bring to the table.”
Some notable partnerships include a venture between Boehringer-Ingelheim and Click Therapeutics on a digital therapeutic for schizophrenia, and a partnership between Sanofi and Happify Health to create a mental health treatment for people with multiple sclerosis. AstraZeneca also developed a digital therapeutic to monitor symptoms in people with breast cancer to gauge treatment response.
Digital therapeutics also have the potential to improve treatment for chronic health conditions, said Hauflaire.
“They are personalized to the individuals. They provide data and insight, 100 data points a minute, which is something that traditional medicines and med devices cannot do,” she said. “It’s well positioned to provide data to individuals and to their provider systems. They’re also low risk, especially when you have a person with a chronic condition, it’s about stacking medications. A digital product does not interfere with those chemicals or biologics in their system.”
France, Belgium, and South Korea, are already working to put this digital therapeutic infrastructure in place and experts hope that the U.S. will follow suit, said Hauflaire. A bill called Access to Prescription Digital Therapeutics Act of 2023, which would expand Medicare coverage to include prescription digital therapeutics, is working its way through Congress.
“But with any piece of legislation it’s very, very slow,” she said.
If advocates successfully make their case, digital therapeutics could become another broadly used tool to improve patient care.
“With the low risk and availability and scalability of digital therapeutic products, I see it becoming the first course of treatment,” Hauflaire said. This technology could also help spur progress toward the holy grail: value-based care.
“With the data provided by digital products we can get there much faster,” Hauflaire said.
In this podcast, Medtech Insight speaks to Andy Molnar, CEO of the digital therapeutics alliance; Joel Morse, CEO and co-founder of Curavit and Owen McCarthy, CEO and co-founder of MedRhythms. The trio discuss the current situation surrounding digital therapeutics, and where they believe they are headed in the coming years.
In this engaging discussion, we delve into the dynamic and evolving world of digital therapeutic (DTx) and decentralized clinical trials (DCTs). We’re joined by industry experts Joel Morse, CEO and Co-Founder at Curavit, and Andy Molnar, CEO at Digital Therapeutics Alliance, offering unique perspectives on this field’s current challenges and innovative strides. Their in-depth knowledge and experience shed light on the complexities and breakthroughs in conducting effective clinical trials in digital therapeutics, a field at the forefront of modern healthcare and clinical trials.
Moe Alsumidaie: How Do You Address Participant Recruitment Challenges in Decentralized Clinical Trials for Digital Therapeutics?
Joel Morse: In digital therapeutics, we adopt extensive web-based recruitment strategies, encompassing social media and email campaigns to target diverse demographics nationwide. This involves creating tailored ads reflecting the specific populations we aim to recruit, such as varying ethnicities, age groups, or genders. Efficiency in gaining IRB approval for these ads is crucial. We’ve also seen success in tweaking these ads throughout the trial to maintain participant engagement and interest.
Andy Molnar: Emphasizing the importance of diversity in trials, we aim to prevent any inherent biases in digital therapeutic tools. This is especially significant in mental and behavioral health areas, where biases can significantly impact treatment outcomes. Digital therapeutics have the potential to treat patients in an unbiased manner, but this requires deliberate efforts in trial design to encompass a wide range of demographics.
Moe Alsumidaie: What is the Impact of Digital Therapeutics in Healthcare?
Joel Morse: Digital therapeutics are revolutionizing healthcare by offering treatments that are more accessible and unbiased, catering to a wide range of patients. The efficient use of digital platforms for recruitment and engagement is a testament to this evolution.
Andy Molnar: These therapeutics are changing the face of healthcare, particularly for conditions like autism, where traditional diagnostics might be biased. Digital therapeutics offer the promise of treating any patient, anywhere, without the biases that might be present in traditional healthcare settings.
Andy Molnar CEO Digital Therapeutics Alliance
Moe Alsumidaie: How Important is Data Management in Digital Therapeutics Trials?
Joel Morse: Effective data management in digital therapeutics trials hinges on meticulous planning. From the outset, it’s essential to know what data will be captured, as realizing midway through a trial that crucial data is missing can be detrimental. The challenge lies not in the technology but in the planning and executing data management strategies, balancing the data collection against participant burden and cost considerations.
Moe Alsumidaie: Can You Discuss the Regulatory Challenges in Digital Therapeutics?
Joel Morse & Andy Molnar: The regulatory landscape for digital therapeutics, especially regarding FDA guidelines and global standards, presents a significant challenge. A particular area of concern is the use of sham apps in trials, akin to placebo controls in traditional drug trials. This is complex and expensive, and there’s ongoing debate about its necessity and effectiveness. Ensuring data sufficiency for not just regulatory approval but also for insurance coverage and reimbursement is another hurdle.
Moe Alsumidaie: How Do You Ensure Patient Safety in Digital Therapeutics Trials?
Joel Morse: Safety in digital therapeutics trials is often enhanced compared to traditional trials. Many of these trials are categorized as low-risk by regulatory agencies. Moreover, the virtual nature of these trials allows for more consistent oversight, better adherence to protocols, and potentially greater participant engagement. This, in turn, leads to higher-quality data and improved safety management.
Andy Molnar: Distinguishing between clinically validated digital therapeutics and the vast array of health apps is crucial for ensuring patient safety. Ensuring that the digital therapeutics being used are effective and safe is essential, especially in scenarios where incorrect guidance could lead to serious health consequences.
Joel Morse CEO Curavit
Moe Alsumidaie: What Lessons Can Be Learned from the Experience of Companies Like Pear Therapeutics?
Andy Molnar: Pear Therapeutics’ journey offers crucial lessons for the industry. They played a pioneering role in digital therapeutics, investing significantly in industry growth and policy development. Despite their bankruptcy, their contributions towards Medicare coverage and regulatory engagement are noteworthy. Their experiences underscore the importance of strategic focus and resource allocation, particularly in navigating market access challenges in digital therapeutics.
Improving diversity, equity, and inclusion (DEI) has long been a goal in clinical trials, in order to ensure that research findings apply to the general US population, among other key benefits. Government agencies related to healthcare have made DEI a priority, with the FDA announcing draft guidance for diversity and inclusion in clinical trials in April 2022. The guidance outlines how the makers of drugs and medical devices, including diagnostic tests, can develop a “Race and Ethnicity Diversity Plan” to ensure better representation of historically underrepresented groups in clinical trials of their products. The requirement to include such a plan for most US clinical trials was made law through legislation passed at the end of 2022. However, developing DEI plans will likely present device makers with a variety of challenges. Rachel Rangel, AuD, a clinical trial specialist at Curavit Clinical Research, discusses IDEA, a new toolkit the company launched in June 2023 to help drug and device makers meet federal diversity and inclusion requirements for clinical trials.
Rachel Rangel, AuD, clinical trial specialist at Curavit Clinical Research.
Q: How does IDEA improve the existing process clinical trial designers would have to go through?
A: Many organizations do not have an established roadmap to improve diversity in clinical trials. Now that the FDA requires a Diversity Action Plan with the submission of new drug and device applications for clinical trials, organizations must have a plan in place to recruit and retain diverse populations or provide justification for why they do not.
Many organizations do not know where to begin. The aim of IDEA is to make it easier for sponsors to create effective and timely plans to ensure that their trials are diverse and equitable from the beginning. IDEA can tackle everything from assessing traditional barriers to entry and gaps in health equity, planning creative recruitment strategies, designing a trial to give participants the utmost autonomy and respect, to tracking enrollment data and being prepared to address gaps in representation.
The IDEA program can be tailored to offer as much or as little support as a sponsor requires. For example, recent work we did for a digital therapeutics customer involved identifying underrepresented populations that would be important to include in their study, taking into account the inequitable burden of the target disease among minority populations, and weighing other key factors to provide a curated list of sites across the country that would have the greatest chance of enrolling and retaining participants from diverse cultural and ethnic backgrounds. This sponsor did not require a full FDA Diversity Action Plan, but they sought our input to make their trial design as inclusive as possible.
Q: What is the importance of DEI planning in clinical research?
A: Diverse participation in clinical research means that, ultimately, we can better determine the effectiveness and safety of medications, medical devices, digital therapeutics, and other forms of treatment across different populations. This leads to a clearer understanding of potential biological, environmental, and behavioral factors that impact the health of different populations, enables discovery of treatments that are more personalized, and most importantly, plays a crucial role in addressing persistent health disparities in the United States.
Planning is absolutely essential to achieving equitable representation within clinical trials. So many times, details that may seem inconsequential at first, such as unnecessarily strict inclusion and exclusion criteria, long travel distance to a site, or inflexible hours can negatively impact the participation of people from underrepresented groups. Forming meaningful connections with community organizations and building trust within communities is not possible overnight—it requires a lot of upfront considerations. Employing diverse and culturally competent site staff can be a significant advantage for recruiting and retaining diverse participants. These are all factors best addressed during the planning stage, rather than while the trial is already underway or has concluded.
Q: Why is DEI planning uncharted territory? What was required prior to this news announcement?
A: DEI planning in clinical trials is less uncharted territory rather than under-explored. Diverse and equitable representation in clinical trials has been often discussed but rarely achieved. One of the reasons for this is most likely that it does require a significant amount of work and time to identify the elements that are required for a trial to be considered a DEI “success.” To get the IDEA toolkit off the ground, we first had to take time to assess our areas of strengths as an organization and areas where support from others would be valuable. We needed to seek out and learn from community partners who are doing the “work on the ground” to get underrepresented populations familiar with and excited about participating in clinical trials. We had to look past our own assumptions about why diversity in clinical trials has been so lacking and instead compile the evidence—reading reports, journal articles, and attending forums and expert panels. Readying the IDEA program required months of dedicated time and preparation work and now ongoing learning that most clinical trial planning teams do not have to spare.
Q: What are the top challenges posed by DEI plan implementation?
A: Operationally, two of the biggest challenges include patient recruitment and retention. Traditional trials at physical sites can limit recruitment to specific geographical areas or only to participants who have the time and resources to travel. It also limits awareness that the trial is even happening—a key reason cited for lack of minority participation in clinical trials. Similarly, patient retention can be hurt if participants cannot sustain long-distance travel. They may not be able to make a site’s limited hours fit in with work or family obligations. Decentralized trials eliminate some of these site-based limitations.
Societal challenges include gaps in awareness and education surrounding participation in clinical trials and hesitancy to engage in clinical trials due to past or current mistreatment by the medical establishment. Historic abuses in the United States such as the Tuskegee syphilis study and the coercive sterilization of Indigenous and other minority women in the 1970s are often cited as reasons for lack of diverse participation in clinical research. This history is crucially important to understand when undertaking research with historically underrepresented communities, but the power of patient education and inviting people to participate should not be underestimated. Many times, a patient’s trusted physician can be an entry point into clinical trials, but in communities that lack access to routine medical care, this is not a viable strategy. Community outreach groups are critical in reaching and forming relationships with communities that may have historically been excluded from clinical trials. Given these challenges, it has never been more apparent that improving diversity and equity in clinical trials requires thoughtful, evidence-based, and purposeful planning from the very beginning. This is where Curavit’s IDEA program can make a major impact.
New FDA Regulations for Diversity and Inclusion in Clinical Trials for 2024
October 17, 2023
In April 2022, the FDA announced that as of 2024, there were new Diversity and Inclusion guidances for clinical trials. Commissioner Robert M. Cliff stated in a press release that “going forward, achieving greater diversity will be a key focus throughout the FDA to facilitate the development of better treatments and better ways to fight diseases that often disproportionately impact diverse communities.” However, higher requirements pose a problem for research groups designing clinical trials, which now must employ more in-depth Diversity and Inclusion planning teams to meet these stringent conditions required to remain FDA compliant. However, there are tools, and more specifically, toolkits that can be applied to help clinical trial staff meet these high requirements.
The importance of representation in clinical trials
Ensuring that the population studied for a clinical trial accurately represents the population actually affected by the condition is vital for interpretation of results. To generate a successful clinical trial, a match between the clinical trial population and condition-affected population is essential. But strategies that are effective at identifying, finding, and enrolling this population are not universal. Particularly in the case of underserved and underrepresented groups, a variety of accessibility barriers can hinder the desired clinical trial representation. For example, ethnic minorities can face language barriers and poverty can reduce an individual’s ability to reach a clinical site due to lack of a vehicle. At multiple stages of the clinical trial, barriers to representation and accessibility must be assessed.
When diversity and inclusion must be taken into account
There is a common misconception that the only time when diversity and inclusion must be taken into account is during the initial, planning phases of a clinical trial. However, there are actually several key areas when diversity and inclusion need to be accounted for including throughout the trial to ensure participant dropout and other alterations throughout do not affect representation overall. In addition to preliminary assessments for representation, continuous assessment of diversity and inclusion rates throughout the trial are needed. These assessments can require extensive resources in terms of time and financial allocations for a clinical research team.
The inclusivity, diversity, and equity in action toolkit
Curavit Clinical Research has recently released their new Inclusivity, Diversity, and Equity in Action (IDEA) toolkit to answer this need of developing and managing diversity action plans. The IDEA toolkit delivers support across five areas during a clinical trial:
Preliminary situational analysis
DEI implementation strategy
Content review
Continuous check-ins
Ongoing optimization
The toolkit includes planning templates to ensure important underrepresented patient populations are included in the clinical trial. IDEA also details how to compile effective strategies to recruit diverse groups of patients for enrollment and identify potential areas where investigators can seek and identify their desired patient populations
Together, tools like IDEA let clinical trial researchers focus on important aspects of a clinical trial without the concern that they have not accurately represented the population affected by the condition being studied. Using the toolkit shows a clinical trial research team when to assess representation and provides templates to provide guidance for reassessing diversity and inclusion criteria and metrics for their clinical trial. Say goodbye to the risk of poor representation by using technology-driven toolkits to plan clinical trials to meet the new mandatory representation guidelines for 2024.
How Companies Are Upping Diversity Among Clinical Trial Participants
October 18, 2023
Pictured: A child flexes his arms for a doctor in a clinic as his mother looks on/Getty
Last year, the FDA released a draft guidance on increasing diversity in clinical trials. Reflecting a surge in efforts to correct the historical exclusion of non-white communities, the guidance also suggests including people with varied gender identities, pregnancy statuses, ages and comorbidities.
Despite increased attention to the need for diversity, it appears that on the whole, clinical trial sponsors are fumbling when it comes to setting and meeting realistic diversity goals: A 2023 report by the IQVIA Institute for Human Data Science showed that the inclusion of Black/African American and Hispanic patients has dropped over the past 5 years, reaching a historic low in 2022.
In a bid to address this issue, the FDA guidelines were folded into the Food and Drug Omnibus Reform Act of 2022 (FDORA), which mandates that clinical trial sponsors submit diversity actions plans to the Secretary of the U.S. Department of Health and Human Services. These plans must lay out the sponsors’ enrollment goals, why they set these goals, and how they plan to meet the goals. As neither the draft guidance nor FDORA prescribe concrete steps, it falls to companies to figure out the details. In such cases, they often rely on clinical trial officers and contract organizations who specialize in diversity, equity and inclusion (DEI). BioSpace spoke with some of these specialists about some key elements of a successful plan.
Integrate DEI from Start to Finish
Most experts agree that diversity and representation must be prioritized from the very beginning of a trial. “The sooner you can do it in the trial planning process, the better because it takes so much more time,” said Rachel Rangel, a clinical trial specialist at Curavit. A contract research organization (CRO), Curavit helps companies determine who they should be enrolling, what has historically stopped these populations from being recruited, and how to best include them in trials today.
Denise Bronner, the director of Diversity, Equity and Inclusion in Clinical Trials at Johnson & Johnson Innovative Medicine, also emphasizes the importance of an early start. For instance, if the initial dosage and safety studies are done on participants who are mostly white and male, then “you really have nothing to inform you of what happens at the next stage,” she said.
Even before beginning trials, recruitment materials should be designed with accessibility in mind. Simple measures like using large font sizes or offering instructions in both written and audio form can go a long way in making trials accessible to a wider swathe of the population, said Courtney Firak, a consultant who helps companies come up with strategies to increase diversity in trials.
Once a diversity plan is set in place, the trial protocol can be optimized to enroll the right participants. This often involves revisiting stringent eligibility criteria like blood markers, which have been shown to restrict participation by members of some groups. For instance, Black/African American people tend to have higher rates of anemia and lower white blood cell counts than white people, rendering many potential participants ineligible for trials that have strict criteria involving these measures. By carefully combing through demographic data and comparing it with the enrollment profiles of old trials, companies can figure out which communities have been left out purely because they did not meet such criteria.
Picking the right study site can also allow people from different groups to participate. This can mean scouting locations in “diversity hotspots” with large numbers of patients, or even in countries outside of the U.S. “These drugs are going into a global market, so you should be thinking about ways to make sure that other countries and other groups are being represented,” Bronner said. Rangel endorses using patient data creatively to find good study sites. For a MedRhythms study on a treatment to help stroke victims walk better, she combined data on the geographic prevalence of stroke with data on populations known to suffer from the long-term effects of stroke. This enabled her to generate a map of potential study sites near people who could benefit from the trial.
One can cast a wide geographical net by conducting decentralized clinical trials, which effectively allow people to participate from their own homes and be monitored through devices or virtual check-ins. By removing the need to visit a trial site, decentralized trials not only expand the geographical reach of the study but allow people with disabilities and demanding responsibilities like caregiving to take part.
A good DEI plan is carried through until the end of, and even beyond, a trial. Every completed trial is a valuable data point that can help companies assess where they have done well and where they have fallen short. Bronner recalls looking back at old trials that fell short of diversity targets to pinpoint where in the pipeline DEI strategies should have been implemented but were not, and learning from those failures. “The trigger, so to speak, that made us think about doing this earlier was looking at those studies consistently and saying, ‘we’re coming in too late,’” she said.
Set Reasonable Benchmarks
One way to assess and facilitate the success of DEI strategies is to set realistic and attainable benchmarks, such as enrolling a target percentage of people from a given community. This can look different for different studies depending on the disease, patient population, geographic location and so on. Bronner recommends drawing from as many databases as possible to get a good sense of patient demographics and disease incidence. Firak further stresses the importance of thinking beyond race and ethnicity, urging companies to gather as much data as possible on intersectional identities that include gender, sexuality and disabilities to account for different perspectives and lived experiences. When collected early on, this data can give sponsors a good picture of the populations they should aim to enroll. “A good diversity goal is if it looks like the population as a whole,” Firak said.
Just this year, trial organizers at Johnson & Johnson realized they had overestimated the difficulty of enrolling diverse trial participants and set too small a goal. After originally aiming for about 35% non-white participants in some of its immunology trials, the company overshot its diversity goal by enrolling close to 50% non-white participants. Organizers also completed some of the trials ahead of schedule and saw that the drop-out rate of non-white participants was no higher than that of white participants. Bronner asserts that this dispels three longstanding myths: that recruiting diverse participants is difficult, that it will take too long, and that non-white participants are more likely to drop out of trials.
Forge Relationships with Communities
One of the most time-consuming aspects of a DEI plan is building relationships with communities, especially those with a history of mistrust in or exclusion by the medical system. A 2019 study showed that a lack of information and trust were critical barriers to participation in clinical trials. One of the ways Johnson & Johnson has tried to address this is by setting up websites like Research Includes Me, which lays out the clinical trial process and how people of color have not been included in the past. Bronner also cautions against “selling” community members a treatment. “You’re really trying to educate them and to be there to answer their questions,” she said. She herself has twice been a speaker at Black Health Matters summits, helping inform community members about Black representation in clinical trials and health disparities in heart disease and multiple myeloma.
A foolproof way of addressing the concerns of specific communities is to simply go to the source and ask people what they need. “It’s a matter of identifying the right partners who have already put that time in, to kind of work with them, get their expertise, and leverage that to your best advantage because we all know that we want to get trials off the ground,” Rangel said.
Firak recommends working with patient advocacy teams who are attuned to the needs of different communities and know how to manage expectations. “It’s likely going to be different strategies for different groups,” she said. “Especially when we’re talking about historically marginalized communities…it will take time and resources to gain that trust.”
Sruthi S. Balakrishnan is a freelance academic editor, science writer and fact-checker based in Santa Barbara, California. She can be reached at sruthisb@sciscriber.com.
Clinical Trial Inclusivity, Diversity, and Equity in Action
In 2022, FDA’s Draft Guidance on Diversity Plans and passage of the Food and Drug Omnibus Reform Act (FDORA) significantly changed the landscape for diversity and inclusion in clinical trials. In this DIA Global Annual Meeting 2023 interview, Curavit President and Co-Founder Dave Hanaman and Clinical Research Business Development Manager Natalia Husby discuss Curavit’s new Inclusivity, Diversity, and Equity in Action (IDEA) service offering with DIA Scientific Programs Associate Director Tamei Elliott. Look for this and similar content in your DIA Global Forum.
Women in Health: Curious, Persistent, Resilient: Natalia Husby, CluePoints
Curavit Clinical Research Business Development Manager Natalia Husby explains the skillset and shares advice that has helped her discover her role as a woman in the life sciences industry. “I went to college, I studied psychology, then over to neuroscience to learn the biological mechanisms behind behavior, and then from there I went into biotech, and now I’m in clinical research,” she explains. “Three skills are important to anyone who excels in science: One is the curiosity and desire to learn because in science there are always new things to learn. The other two go hand in hand: Persistence and resilience, because so many things go wrong in science, in life, in business, and it’s important to not get discouraged when things don’t go according to plan. In those opportunities where things don’t go as expected, learn from those experiences, and drive yourself forward.” Look for this and similar content in your DIA Global Forum.
Curavit Chosen as Contract Research Organization for MedRhythms Clinical Trial
Company expected to research patient engagement, response durability, and health economics of new medical device.
Curvait Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), revealed in a company press release that it was chosen for a study of MR-001, MedRhythms’ neurorehabilitation system designed to improve walking and ambulation in adults with chronic stroke walking impairments. As part of the collaboration, Curvait will be responsible for managing all aspects of MedRhythms’ hybrid decentralized clinical trial (DCT) – from protocol finalization and Institutional Review Board (IRB) approvals to patient recruitment, testing at physical sites, remote site and patient monitoring and healthcare economics and outcomes analysis.
“As innovators in healthcare, it’s essential to show that new technologies not only have the power to transform patients’ lives but are also economically prudent. Health economics research quantifies the long-term financial impact for patients, providers, and payers,” said Owen McCarthy, president, co-founder, MedRhythms. “Curavit’s tech-enabled approach to research lets us launch quickly while delivering a premier experience for everyone involved. As important, the study will be open to participants nearly nation-wide, thanks to Curavit’s virtual site solution, patient recruitment process, and smart strategies for collecting real-world healthcare economics data.”
Reference: MedRhythms Selects Curavit as its Contract Research Organization (CRO) for a Chronic Stroke Decentralized Clinical Trial. PR Newswire. September 20, 2023. Accessed September 25, 2023. https://www.prnewswire.com/news-releases/medrhythms-selects-curavit-as-its-contract-research-organization-cro-for-a-chronic-stroke-decentralized-clinical-trial-301932835.html
MedRhythms sounds out Curavit to study auditory stimulation tech on stroke patients
Curavit, a virtual contract research organization, has been signed up by MedRhythms to run a study of its technology aimed at aging adults with walking impairments as a result of a stroke.
Dubbed MR-001, the system uses MedRhythms’ rhythmic auditory stimulation to improve walking and ambulation in adults who have suffered a chronic stroke, the company said in a Sept. 20 press release. The system involves auditory-motor entrainment during which the brain subconsciously synchronizes to an external auditory cue like music.
The two companies, which began working together in June, aim to enroll 225 participants for the 12-month trial by the end of the year. The OrcHESTRAS study is partly designed to generate evidence of the product’s ability to reduce the financial impact of the condition on the U.S. healthcare landscape.
“We are honored to work with MedRhythms to manage such an important study of an innovative neurorehabilitation system to help stroke patients improve walking without invasive therapy or pills,” Curavit CEO Joel Morse said in the release. “We believe it is going to become increasingly important for [digital therapeutics] companies to capture health economics data to enable broader market access.”
Curavit launched in late 2019, just months before the onset of the COVID-19 pandemic. Disruptions caused by the crisis initiated a global embrace of decentralized clinical trials that have continued to gain popularity.
Curavit VCRO chosen to manage study of MedRhythm’s neurorehabilitation system for stroke patients
A study of MedRhythm’s MR-001 neurorehabilitation system, designed to improve walking and ambulation in adults with chronic stroke impairment, will use Curavit Clinical Research as its virtual contract research organization (VCRO).
New York- based decentralized contract research organization (CRO) Curavitannounced MedRhythms’ selected the company as its CRO of record. Importantly this news points to one of the first digital therapeutics (DTx) trials to focus on capturing evidence on the product’s financial impact on the U.S. healthcare system. This kind of study, which is also capturing health outcomes data, is increasingly vital to DTx companies struggling to secure broad market access to its products.
Right now, there is no infrastructure and a lack of private and government insurance coverage for many prescription and non-prescription digital therapeutics although they are proven to be a cost-efficient, less invasive form of treatment.
Pear Therapeutics’ bankruptcy was larging a result of these challenges. Akili Therapeutics, in response to this issue, has pivoted its go-to-market model by going direct to consumers, selling at a lower price point than a prescription product but circumventing insurers.
MedRhythms is committed to getting the financial validation of its product to help increase payer coverage and get its novel neurorehabilitation system to patients in need as fast as possible. As a specialist in DTx, Curavit understands and that is why they were selected by MedRhythms on this very important project that could lay the blueprint for more DTx companies to follow with the goal of driving market access.
TrialSite has engaged with Curavit in 2021, at the start of the venture’s journey. In an interview with President and Chief Commercial Officer Dave Hanaman, TrialSite learned more about the nascent decentralized research company’s business model, and value proposition.
According to TrialSite’s founder Daniel O’Connor, “Curavit’ s founders have deep expertise, pedigree and vocational certainty in the field of pharmaceutical-related services. They founded another services company that was ultimately acquired by Merck.”
That company was C3i, a business process outsourcing leader in healthcare. That company worked with several of the largest pharmaceutical companies to support e-clinical trials applications for example O’Connor shared.
Joel Morse, Chief Executive Officer, and Hanaman complement each other well. Both are obsessive about high quality delivery in complex, difficult regulatory environments and the Curavit team appears to embrace that founder’s culture.
With initial fundraising and about 30 employees, now the company seems poised to grow.
The Study
With the latest news Curavit reports to TrialSite that the company will power the OrcHESTRAS (Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation) study – one that is a prospectively enrolled study, with a novel design that focuses on evidence generation and exploration of the product’s impact on reducing financial impact on the U.S. healthcare landscape.
Curavit is responsible for managing all aspects of MedRhythms’ hybrid decentralized clinical trial (DCT) – from protocol finalization and Institutional Review Board (IRB) approvals to patient recruitment, testing at physical sites, remote site and patient monitoring and healthcare economics and outcomes analysis. The partnership between the companies began in June 2023, and the 12-month trial aims to enroll 225 participants by the end of the year.
“As innovators in healthcare, it’s essential to show that new technologies not only have the power to transform patients’ lives but are also economically prudent. Health economics research quantifies the long-term financial impact for patients, providers, and payers,” said Owen McCarthy, President and co-founder of MedRhythms. “Curavit’s tech-enabled approach to research lets us launch quickly while delivering a premier experience for everyone involved. As important, the study will be open to participants nearly nation-wide, thanks to Curavit’s virtual site solution, patient recruitment process, and smart strategies for collecting real-world healthcare economics data.”
MR-001 is based on Rhythmic Auditory Stimulation (RAS), a clinical intervention utilizing the mechanism of auditory-motor entrainment (“entrainment”). During entertainment, the motor and auditory systems in the brain subconsciously synchronize to an external auditory cue, such as music.
“We are honored to work with MedRhythms to manage such an important study of an innovative neurorehabilitation system to help stroke patients improve walking without invasive therapy or pills,” said Joel Morse, CEO and co-founder of Curavit. “We believe it is going to become increasingly important for DTx companies to capture health economics data to enable broader market access.”
Call to Action: Sponsors that are in the digital health and related space should do an assessment of Curavit’s capabilities.
MedRhythms Selects Curavit for MR-001 Trial in Stroke Impairment
Curavit is responsible for managing all aspects of MedRhythms’ hybrid decentralized clinical trial.
Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), was selected for a study of MR-001, MedRhythms’ neurorehabilitation system designed to improve walking and ambulation in adults with chronic stroke walking impairment. The goal of the study is to further characterize the long-term clinical benefits of MR-001 beyond what has been established in a multi-center, randomized clinical trial. This will also include evaluating patient engagement and therapeutic response durability.
The study, known as OrcHESTRAS (Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation), is a prospectively enrolled study, with a novel design that focuses on evidence generation and exploration of the product’s impact on reducing financial impact on the U.S. healthcare landscape.
Curavit is responsible for managing all aspects of MedRhythms’ hybrid DCT, from protocol finalization and Institutional Review Board (IRB) approvals to patient recruitment, testing at physical sites, remote site and patient monitoring and healthcare economics and outcomes analysis.
MR-001 is based on Rhythmic Auditory Stimulation (RAS), a clinical intervention utilizing the mechanism of auditory-motor entrainment. During entrainment, the motor and auditory systems in the brain subconsciously synchronize to an external auditory cue, such as music.
“As innovators in healthcare, it’s essential to show that new technologies not only have the power to transform patients’ lives but are also economically prudent. Health economics research quantifies the long-term financial impact for patients, providers, and payers,” said Owen McCarthy, president, and co-founder of MedRhythms. “Curavit’s tech-enabled approach to research lets us launch quickly while delivering a premier experience for everyone involved. As important, the study will be open to participants nearly nation-wide, thanks to Curavit’s virtual site solution, patient recruitment process, and smart strategies for collecting real-world healthcare economics data.”
“We are honored to work with MedRhythms to manage such an important study of an innovative neurorehabilitation system to help stroke patients improve walking without invasive therapy or pills,” said Joel Morse, CEO and co-founder of Curavit. “We believe it is going to become increasingly important for DTx companies to capture health economics data to enable broader market access.”
Improving Health Equity and Diversity Throughout the Life Sciences
Since 2020, diversity, equity, and inclusion (DE&I) has been a prime area of attention within healthcare and the life sciences. For one, the pandemic put a spotlight on the disparity within clinical trials—in 2020 the FDA found that 75% of trial participants were white, 11% were Hispanic, 8% were Black, and 6% were Asian. Furthermore, the rise of the Black Lives Matter movement at the time forced organizations in all industries to take a closer look at their DE&I efforts and inspired some to do better and go beyond attempts that often only paid lip service to improving diversity.
Inequity within healthcare overall has been a long-standing issue in need of solutions. Just some of the statistics found by KFF analysis include: American Indian and Alaska Native (AIAN) and Black people had a shorter life expectancy at birth (65.2 and 70.8 years, respectively) compared to White people (76.4) as of 2021, Black infants were more than two times as likely to die as white infants as of 2021, and the age-adjusted mortality rates for diabetes in 2021 for AIAN, Native Hawaiian and Other Pacific Islander (NHOPI), and Black people were twice as high as the rate for white people.
As life sciences companies look for ways to improve DE&I both within their organizations and in healthcare as a whole, PM360 turned to 10 experts in the space to ask them how. Specifically, we wanted to know:
What steps should companies within the life sciences industry take to make a greater impact in improving diversity and health equity in areas including clinical trials, drug development, diagnosis, access to medication, marketing, data analysis, health literacy, etc.? What is the most important thing companies can do to make the biggest impact?
What organizational changes do companies have to make to ensure they are better equipped to recognize the areas where they are failing to properly reach underserved groups?
How can companies gain a better understanding into the needs of underrepresented and underserved groups to develop programs, approaches, products, strategies, etc. that address the issues and social determinants most impacting their healthcare? In your work in this area, what have you found to be the most surprising need of a specific group that the industry has not been addressing?
What partnerships can companies form outside of their organizations to help boost health equity more broadly across the healthcare ecosystem? Do you have any examples of unique partnerships that are making significant progress? What have been the keys to these partnerships’ success?
Natalia Ledo Husby
Business Development Manager
natalia.ledohusby@curavitclinicalresearch.com
Increasing diversity in clinical trials is not a one-solution problem. It requires investment, innovation, and community building. However, companies can take some concrete actions right now to create a culture that fosters diversity and health equity.
1. Educate all employees about the importance of diversity in clinical trials and potential barriers that contribute to unequal access. Many people think they understand but if they have never been in the shoes of someone who has experienced a history of injustice, it can be difficult to fully comprehend. One good resource is the National Institute on Minority Health and Health Disparities (NIMHD).
2. Evaluate existing and new protocols to see if they make it needlessly difficult for historically underrepresented groups to participate in the trial. Prioritize accessibility in all protocol designs and, at the same time, create an action plan to proactively engage with underrepresented communities. Educate them about the importance of clinical trials and encourage informed participation.
3. Leverage today’s novel recruitment strategies including social media outreach and AI-based recruitment. Partner with local community organizations and leaders, pharmacies, and healthcare clinics that have the trust of their patients. Also, ensure all trial materials are comprehensible for people with varying degrees of health literacy and/or language proficiency.
Population representation in trials is a thorny problem to solve, especially for early-stage life sciences and digital therapeutics companies without major resources to invest—but even in larger companies no one seems to know where to start. Yet it is crucial we do solve it—not just for health equity but for the legitimacy of clinical research. If trials do not include people from every relevant demographic, the data is skewed and the resulting therapies won’t have the same effect for everyone.
Rigorous Data Are Key to Convince Payers, Investors in the World of Digital Therapeutics
Pear Therapeutics was once regarded as a digital therapeutics pioneer, but its spiral into bankruptcy has the industry searching for the best path forward. While some favor going direct to consumers, others say the solution is in generating more robust clinical trial data to persuade hesitant payers.
The most common and easiest way to take medicine is by swallowing a pill. For a new class of therapies, dosing is even easier—just a few finger taps on a touchscreen. The now-defunct Pear Therapeutics was a pioneer among companies developing such software-based medicines.
Digital therapeutics engage users with apps and tasks that retrain and rewire the brain as a way of treating a range of diseases. This treatment is usually done alongside the standard of care, which can include drugs. That’s different than health and wellness apps that provide users with a wealth of information but cannot make therapeutic claims.
Boston-based Pear won the first FDA authorization to bring prescription digital therapeutics to the market in 2017 for substance use disorder. It was an interactive software that provided app users with lessons for achieving and maintaining abstinence. Later, Pear commercialized apps for opioid use disorder and insomnia. Other companies have followed, receiving the FDA’s go-ahead in indications such as mental health disorders, obesity, heart disease, and more.
Despite being first to market, Pear struggled as a commercial-stage company. In a widely read LinkedIn post, Pear CEO Corey McCann said doctors prescribed Pear’s products and patients successfully engaged with them. The problem, as he saw it, was that payers denied coverage. With cash reserves dwindling and no prospects for additional financing, Pear filed for bankruptcy protection and auctioned off parts of its business in June for pennies on the dollar.
Pear’s high-profile failure raises questions about the future of digital therapeutics. Almost everyone says this sector needs to produce more data to ease the financial risk that investors perceive and to persuade payers to reimburse these technologies. There’s less agreement on how to generate the data.
Three years ago, digital therapeutics was one of several sectors that saw an investment boom from the Covid-19 pandemic, said Rahul Rakhit, a research analyst at LifeSci Capital. Pitchbook recorded $1.5 billion in venture capital investment in digital therapeutics across 54 deals in 2019 and $1.3 billion across 49 deals in 2020.
It’s a different story today, as companies struggle to raise capital. Pear might be the first of several digital therapeutics firms to fall, Rakhit said. Alternatively, the financial challenges could spark consolidation that results in a smaller but stronger field.
“I’m still bullish on this category,” Rakhit said. “It addresses a number of important unmet needs, especially post Covid—demand for healthcare that outstrips the resources we have available, rural areas where people don’t have access. This democratizes care in a lot of ways. It will take time to see what works, what doesn’t.”
Is Direct to Consumer the Prescription for Success?
The digital therapeutics sector breaks down to two camps: prescription and non-prescription. The prescription route is akin to traditional drug development, where a company raises several rounds of funding and takes a product through clinical development and regulatory review, said Rick Anderson, president of digital health company DarioHealth. The other pharma-emulating piece of this model is a partnership with a pharmaceutical company. In biotech, most companies reach late-stage development in partnership with a big pharma company that has the experience and the resources to steer a drug through FDA review and commercialization. Pear had a big pharma partner (Novartis) but that deal fell apart. Dario has a big pharma partner (Sanofi), but is taking a different approach to commercialization.
Dario deliberately chose a direct-to-consumer route, Anderson said. The company began as a diabetes care company. Dario Evolve is its metabolic software offering, an app that helps users track and manage their diabetes, blood pressure, and weight. The company’s offerings now also address musculoskeletal conditions (Dario Move) and mental health (Dario Elevate).
Dario makes its software directly available to consumers but it attributes most of its revenue growth to employers and health plans that make the software available to their members. While this approach means the company isn’t conducting randomized controlled clinical trials, Dario still generates data on clinical outcomes. In 2022, Dario inked an agreement with Sanofi under which the companies co-promote some of Dario’s multi-condition therapeutic, which spans diabetes, hypertension, weight management, musculoskeletal health and behavioral health. Those products and services will create new insights, some of which will be used to develop new products and services. Sanofi committed $30 million over the course of the alliance, during which the companies are conducting studies to generate data about the impact of digital therapeutics.
“I do believe the demand for evidence is going up and you’re going to see more studies,” Anderson said. “But I don’t think the FDA stamp of approval is the level of evidence people are looking for.”
Pear was partnered with Novartis, which had previously invested in the startup’s financing rounds. The pharma giant formally inked a schizophrenia and multiple sclerosis R&D partnership with Pear in 2018. By that point, Pear had received FDA marketing authorization for reSET in substance use disorder, a regulatory decision that marked the first time the agency permitted the marketing of a mobile app for this indication. In late 2018, Pear received FDA clearance for reSET-O—essentially reSET for opioid use disorder. Pear had a separate agreement with Novartis’s Sandoz subsidiary covering the commercialization of both reSET and reSET-O. In 2019, Sandoz terminated the deal.
Left to commercialize its digital apps on its own, Pear, which became public in 2021 through a SPAC merger, pointed to growing prescription numbers quarter to quarter. The problem was that half of those prescriptions weren’t filled and many payers failed to reimburse them because medical codes don’t exist, said Joel Morse, CEO and co-founder of Curavit Clinical Research, a contract research organization that specializes in decentralized clinical trials for digital therapeutics. Difficulty securing insurance coverage is not unique to Pear, but Curavit President and Chief Commercial Officer Dave Hanaman sees legislation as one way to drive change for all digital therapeutics companies. The Access to Prescription Digital Therapeutics Act of 2023 would expand Medicare coverage to include coverage of software-based treatments. Broader payer coverage should follow, Hanaman said.
LifeSci Capital’s Rakhit said payers are still tiptoeing around digital therapeutics, trying to understand what data they need to see. Investors are also uncertain about the space. In Pear, they saw a company that despite reporting prescription growth was burning through a lot of cash and showed no clear path to profitability. Rakhit said it’s not a question of whether digital therapeutics work, but rather how best to use them. For psychiatric conditions, the safety benefit of a digital therapeutic is attractive. While psychiatric drugs introduce many side effects, there’s almost no safety risk to a patient downloading an app to try it out, he said.
Going directly to consumers may be appropriate in some cases, Rakhit said. Akili Interactive’s EndeavorRx video game first received FDA clearance in 2020 as a prescription treatment for attention deficit hyperactivity disorder in children ages 8 to 12. On the heels of positive clinical trial data in adults, Akili last month announced availability of a non-prescription version for those 18 and older.
A non-prescription ADHD digital therapeutic for adults makes sense because adults tend to self-treat more than children do, Rakhit explained. While this OTC version of EndeavorRx will generate less revenue than a prescription product, it will enable Akili to cast a wider net that captures a broader swath of the population. Further, wider use generates more data, which is what payers and investors want to see. However, the direct-to-consumer strategy may be inappropriate for indications such as substance use disorder, the realm where Pear was playing with reSET and reSET-O. When it comes to drug abuse, physicians are central to patient treatment, Rakhit said.
Parsing Pear’s Clinical Trial Data
Payer concern about reimbursing for Pear’s apps might be related to the quality of the available data. The clinical trials used to support the regulatory applications were not done by Pear. In fact, those trials did not even test the Pear apps. Pear’s reSET and reSET-O incorporate technology licensed in 2015 from a company called Red 5 Group, which owns an app called Therapeutic Education System, or TES, according to Pear regulatory filings. This software has 62 interactive modules designed to help the app user achieve and maintain abstinence, compared to reSET, which has 61 modules.
Pear’s FDA submission for reSET was based on an open-label study conducted by the National Institute on Drug Abuse, the company said in documents submitted to the FDA in 2016. The 399 participants in the trial were evaluated on the desktop version of TES rather than the mobile version of reSET.
FDA clearance for reSET-O in opioid use disorder was based on that app’s equivalence to reSET. A clinical trial supported this submission, but like the prior study referenced by Pear, this one evaluated patients who used TES, not reSET-O. TES’s 12-week clinical trial, which was also done in collaboration with the National Institute on Drug Abuse, enrolled 507 participants randomly assigned to receive treatment as usual or treatment as usual and TES. In study results published in 2014 in The American Journal of Psychiatry, the authors acknowledged limitations that include the impossibility of separating the effects of the computerized approach from other aspects of care. The authors also noted that with longer-term follow-up, the superiority of TES over treatment as usual was not sustained.
Drug price watchdog group the Institute for Clinical and Economic Review (ICER) panned the short duration of the study and the lack of a sham control arm. ICER added that TES’s differences from reSET-O could mean its test results may not be applicable to the Pear app. Pear responded by pointing to real-world evidence in peer-reviewed studies that showed reSET-O reduced the need of app users to turn to healthcare resources, leading to measurable dollar savings compared to standard of care. But ICER raised questions about these data too, and called for more robust and rigorous research.
David Klein, CEO of Click Therapeutics, said that if Click or any other digital therapeutics company develops a drug-like product that makes drug-like claims, the supporting clinical trials must generate the same level of evidence asked of any biotech company. In Klein’s view, Pear lacked sufficient evidence from randomized controlled clinical trials.
“If you put reSET-O with that evidence into a pill, I don’t think payers would be reimbursing for that either,” he said.
Click’s prescription-based approach may differ from Dario’s consumer-focused strategy, but one thing that they have in common is a relationship with Sanofi. Sanofi’s venture arm was one of the early investors in Click. Klein describes Click’s strategy as a hybrid one in which some programs are partnered with a larger company that can help with clinical development and commercialization. A depression digital therapeutic is in development under a partnership with Otsuka Pharmaceutical and two schizophrenia product candidates are partnered with Boehringer Ingelheim. But a Click migraine digital therapeutic in Phase 3 testing remains unpartnered, and Klein said that’s intentional. Click aims to commercialize some assets on its own.
Felix Lee, medical head, digital healthcare, for Sanofi U.S., was unavailable for an interview to discuss the pharma giant’s digital strategy. But in an emailed statement, he said the integration of healthcare and technology can give people tools to improve their health, and Sanofi sees digital therapeutics as a key pathway to improve patient care beyond medicines.
“We know that health outcomes are not only determined by medical care but also by behavior, socioeconomic and other factors that can be addressed with personalizing interventions, which can be especially important in chronic disease management,” Lee said.
A Digital Player Finds Footing After FDA Nod
A new digital therapeutic is on track to enter the market soon, and it will be a prescription product. Better Therapeutics received FDA authorization earlier this month for AspyreRx, a type 2 diabetes mobile app that digitizes cognitive behavioral therapy. Using the app leads to behavioral changes intended to change the course of the disease. Better’s application was based on results from a Phase 3 study that showed treatment with AspyreRx, alongside standard care (including diabetes medications), led to reductions in hemoglobin A1C, a biological indicator of blood sugar levels.
Similar to Pear, Better has had financial struggles. A corporate restructuring earlier this year led to layoffs. The company’s stock price sank to the point of triggering a delisting warning. But the regulatory authorization of AspyreRx along with the supporting data from a pivotal trial give Better firmer ground to stand on as it negotiates commercialization opportunities, CEO Frank Karbe said during a conference call to discuss the FDA decision. The company’s options include an alliance with a larger partner or raising non-dilutive financing by striking a deal for the product’s royalties.
Discussions with payers are ongoing, and having clinical data from a Phase 3 randomized controlled clinical trial resonates with them, Karbe said. The discussions include value-based agreements, deals in which reimbursement is tied to measurable patient outcomes. The clinical data provide a framework for those discussions. Karbe said these data are key to the company’s commercialization strategy.
“Our product is authorized as a class 2 medical device, which we believe is critically important to ensure we and others meet specific standards for quality, safety, and effectiveness,” he said. “It is also an important prerequisite to obtain broad payer coverage and gain the trust of providers and patients, all of which are important drivers for adoption.”
Wall Street Journal Pro
Media Coverage | Outsourcing Pharma
August 1, 2023 Joel Morse
Curavit CEO and co-founder, Joel Morse, provided background information for the important news article below for the Wall Street Journal Pro section. Read on to learn more about some of the issues confronting the digital therapeutics industry.
Good day. Startups that develop software-based disease treatments are devising strategies to overcome reimbursement obstacles that have hampered the emerging industry.
Digital therapeutics, often delivered through an app, have attracted venture capital in part because of their potential to extend the reach of medical care and reduce inequalities. The global digital-therapeutics market was valued at $5.09 billion in 2022, according to market tracker Grand View Research.
Because these treatments are new, securing reimbursement is often a slow process. Pear Therapeutics, a pioneer in the sector, filed for bankruptcy in April because of this challenge. Until there is a robust infrastructure for reimbursement, commercialization will be challenging, said Autumn Brennan, director of marketing and communications for Digital Therapeutics Alliance, a nonprofit trade group.
A bipartisan bill in Congress, the Access to Prescription Digital Therapeutics Act, would require the Centers for Medicare and Medicaid Services to establish a payment methodology for these treatments.
Companies are also taking their own measures. Startup Click Therapeutics is developing prescription digital treatments for migraines, schizophrenia and other conditions with the same clinical rigor as a drug, which should encourage adoption, said co-founder and Chief Executive David Klein.
“Our approach takes into account that evidence of efficacy will be required for new medicines, and digital therapeutics shouldn’t receive any special treatment,” Klein said.
Another strategy is to deliver digital therapies directly to insurers, employers, and other customers without the need for a prescription. One company taking this approach is publicly traded DarioHealth, whose platform is designed to help people manage chronic conditions between doctor visits. Putting a doctor in the middle of the process adds a barrier for patients, said President Rick Anderson.
Curavit: Tackling under representation with the right balance of patient care, science and business
New guidelines have been issued by the FDA called Diversity Plans to Improve Enrollment of Participants from Underrepresented Racial and Ethnic Populations in Clinical Trials. Curavit was ahead of the game with its plans, find out how.
According to Joel Morse, CEO and co-founder of Curavit Clinical Research, several factors influence today’s outsourcing landscape, including available resources, regulatory changes, and advancements in technology.
Episode Details:
Our Guest: Joel Morse, CEO at Curavit Clinical Research
What you’ll get out of this episode:
Joel’s background
Curavit Overview
CRO and virtual clinical site services for clinical trials
Traditional vs. Decentralized Clinical Trials
What the future of this space looks like?
A Crossroads for the Digital Therapeutics Industry. Now is the Time to Act
According to Joel Morse, CEO and co-founder of Curavit Clinical Research, several factors influence today’s outsourcing landscape, including available resources, regulatory changes, and advancements in technology.
Recent events can provide digital therapeutics companies with clear lessons for the future.
When four companies purchased the remnants of Pear Therapeutics at auction for $6.05 million in May, it marked the unfortunate final chapter in the demise of a pioneer in digital therapeutics (DTx). Pear’s bankruptcy, and ultimate dismantling, have sent shockwaves through the industry and laid bare some of the persistent challenges facing the DTx sector along its winding path forward. But the lessons that can be learned from the loss of Pear will provide us with an important opportunity to better understand the calibrations that companies must make to ensure that digital therapeutics can have a viable and sustainable future.
Despite remarkable growth and the regular development of groundbreaking and potentially life-changing therapies, the fall of Pear might be the clearest indication yet of the challenging headwinds facing the industry. Clearly, intriguing technology is not enough to ensure that DTx companies are successful. Like any pharmaceutical company, DTx firms require large amounts of capital as well as access to markets and reimbursement channels to ensure their success. Despite appearing to be at the very tip of the spear when it comes to the future of healthcare, the ‘if you build it, they will come’ mentality often employed by DTx companies is not enough to ensure sustainability.
The industry is at an important inflection point and it is time to refocus our efforts to ensure the continued vitality of the DTx industry in the years ahead. Through an honest and reasoned examination of Pear’s situation, we can glean valuable information, as well as develop a potential roadmap for current and future DTx companies to follow as they navigate the bumpy road ahead.
Facing an Uncertain Economy
While digital therapeutics has been the fastest growing sector in healthcare for several years and has benefited enormously from investors looking to gain a foothold into a promising and potentially lucrative market, clouds have been gathering on the horizon.
“Market conditions over the last two years have challenged many growth-stage companies, including us,” Corey McCann, the CEO of Pear, wrote in a LinkedIn post last April, when Pear filed for bankruptcy.
Pear admittedly made a few economic missteps. For starters, the company spent nearly $150 million on a broad pipeline before market validation of its first product. And, amidst a tightening financing environment, Pear went public via a SPAC at a high valuation, only raising half the capital it expected ($200M vs $400M). This did not afford the company enough time to establish reimbursement, given their burn rate of $35M per quarter.
From rising inflation and interest rates to supply chain challenges, the stagnating, post-pandemic economic environment has blunted some of the eagerness for investment in DTx companies. Additionally, mergers and acquisitions have fallen, and lending options have become more challenging, particularly for start-ups.
Overall, venture capital funding is trending downward in 2023 and many DTxcompanies—still in the early stages of development—find themselves cash-strapped and unable to allocate the necessary funds for such vital activities as clinical research and commercialization. For instance, Akili (one of only two DTx companies to share its financials publicly) brought in nearly $20 million in revenue in 2019, while in 2020 it only brought in about $4 million, most of which was from an ongoing licensing agreement with Shionogi & Co. to commercialize its products in Taiwan and Japan. In addition, the recent failure of Silicon Valley Bank, as well as the precarious stability of a few other financial institutions, has only contributed to economic uncertainty.
The tides have turned from the financial boom of 2020 (with 73 life sciences firms collectively raising $22 billion), and that presents challenges for the foreseeable future. DTx companies – many of which are startups – will need to batten down the hatches to ensure that they can weather the potential storms ahead. Now more than ever, these companies will have to focus on the economic viability of their products, rather than simply relying on their value and innovation.
Reimbursements are One Key for Success
Regardless of the current economic environment, the outlook for digital therapeutics remains bright, with several conditions that seem to point toward future success. For example, as more of the digitally native Gen Z enters the healthcare marketplace, the appetite for digital products only stands to grow. This, coupled with the accelerating effect that COVID-19 had on the overall comfort-level that most people have with technology in healthcare, would seem to present a positive outlook for DTx companies in the long term.
Yet, despite the growing market and an ever-increasing favorability among patients and care providers toward technology in healthcare, overall adoption rates of DTx products remain stubbornly low. While the global DTx market is poised to reach more than $14.5 billion by 2028, the FDA had only approved nine PDTx categorized as Class II devices as of December 2022. The first was reSET, a PDTx for treating substance use disorder, developed by the now-bankrupt Pear Therapeutics. Several DTx companies tell us that prescriptions are lower than expected right now. Part of the reason for this stagnation is because there is no framework in place for the payer evaluation process.
Clinicians not only want to see trial data and real-world evidence for confidence in PDTx safety and efficacy, but they also want a clear, straightforward claims process and reimbursement pathway for payment. A physician serving on a webinar panel explained, “If one payer has a PDTx as a medical benefit, another as a pharmacy benefit, and another as this ‘new thing that might happen,’ then my office isn’t going to be able to manage it.”
This unfortunate reality has put all DTx companies at an extraordinary disadvantage, which many—including Pear—find to be a barrier to success.
“The advancement of digital therapeutics requires a paradigm shift in how medical interventions are delivered and integrated through a complex infrastructure,” said Autumn M. Brennan, director of marketing and communications at the Digital Therapeutics Alliance (DTA), a global non-profit trade association. “It’s an absolute necessity that we clear the path by collaborating with policymakers, regulatory bodies, payors, patients, and caregivers. All their input is imperative for us to build systems and standards for healthcare that are fair and equitable.”
In many ways, DTx companies find themselves ahead of the marketplace. And while this speaks to their extraordinary level of innovation, it has also created the unenviable situation of having far too many payers who are unequipped to reimburse them appropriately—or at all—for their products. The entire healthcare ecosystem needs to come together to rectify this situation or else the innovation, improved care, better access, and potential cost savings that might be gained from the innovations created by DTx companies might never come to fruition.
“The lack of a defined benefit category and the patchwork of commercial coverage options have meant too few people—and especially those with public coverage—are benefiting from DTx therapies,” Brennan said.
The Access to Prescription Digital Therapeutics Act of 2022, which was introduced in the Senate last year, aims to change this ineffective structure. The legislation would create a new benefit category for digital therapeutics and ensure permanent coverage and reimbursement of digital therapeutic products by Medicare and Medicaid. This would help to pave the way forward for DTx companies to see more reimbursements and earn a fair return on their considerable investments toward improving care and access to care.
Accessing a Hard-to-Access Market
As with any company, DTx firms often stake their claims around the singularity of their products. And while it is easy to understand this tactic, the blinding light of an exciting new technology can often distract companies from their most fundamental responsibility: Producing a product that has economic value. It is more likely that health plans and payers will take notice and markets will open with a financially viable product.
Last year, Pear reported that 45,000 prescriptions were written for its products, yet only about half of these were filled and the company was only reimbursed for a mere 41% of those filled prescriptions. Despite its attempt to follow the rules created for more traditional pharmaceutical companies, this poor adherence and reimbursement record proved disastrous for Pear and has had a negative residual effect on all companies in the DTx sector.
Regardless of how impressive the technology is, the products that have longevity—and, ultimately, profitability—also have an unwavering focus on health economics. Clinical trials can be the path to demonstrate the health economics as well as efficacy and safety of DTx, but they are expensive. And as the pandemic-related loosening of regulatory requirement restrictions gets tightened once more, DTx companies are facing an even steeper challenge when it comes to the commercialization of their products.
If companies are not reimbursed enough for their prescription digital therapeutics, low returns could stifle innovation, said Marisa Greenwald, healthcare partner at consultancy EY-Parthenon.
“Pear’s situation really highlights the need for more transparency and clarity around what it requires for companies to bring a product to market,” Brennan said. “Digital therapies have a big educational learning curve, not only for customers but also for practitioners.”
In a provider survey, Decimal.health found that even though fewer than 22% of providers had prescribed a DTx product, more than 87% indicated that they would be interested in prescribing DTx in the future. The question is: what is the best path to profitability? Some DTx companies are reevaluating regulatory strategies and considering alternative paths, including direct-to-consumer (DTC) routes, to commercial success.
In a DTC model, the product would be sold on websites and pharmacies the same way you might purchase health and wellness products, vitamins, and ‘cosmeceuticals.’ This strategy eliminates the per-unit sticker price, but at the cost of losing FDA credibility. If you can get treatment without a prescription, the product price plummets so the seller must make up for that gap with significantly greater sales volume. DTx companies are left facing a dilemma to choose between two less-than-ideal options:
Pursue the FDA approval process even though they are uncertain about reimbursement
Commercialize directly to consumers under the Federal Trade Commission (FTC) without payer reimbursement
Clearing a New Path to Success
The road to success begins with clarity. We must continue to lobby for universal standards on how digital therapeutics are defined and establish a common regulatory and coverage infrastructure to support broader access to these innovations.
More broadly, the industry should invest in educating practitioners (and patients) about the value and use of digital therapeutics the same way traditional pharmaceutical companies keep physicians up to date on their scientific developments.
“We’re seeing big gaps with digital therapeutics. Students graduating from medical school right now absolutely need to understand digital therapeutics,” Brennan concluded. “It’s the future of medicine and the next wave of practitioners need to understand the power of digital therapeutics and how it can serve the communities that they are treating.”
In many ways, DTx companies have been a victim of their own successes. By producing such unique and groundbreaking products, they have gotten ahead of the often slow moving and archaic healthcare regulatory system. Yet now more than ever, the DTx sector needs to come together to create a new pathway forward that will help to ensure its long-term success so that consumers can benefit from these remarkable innovations for years to come.
According to Joel Morse, CEO and co-founder of Curavit Clinical Research, several factors influence today’s outsourcing landscape, including available resources, regulatory changes, and advancements in technology.
“With these factors in mind, we are seeing an increased reliance on outsourced expertise in virtual/remote clinical trial design and execution to keep costs down, along with experience in recruiting and enrolling a diverse trial participant population to meet new regulatory requirements and improve patient care for all.”
“It’s a big question and I think you could come at it from many different angles, but if we look at what we see at Emmes as the most promising growth areas then we continue to see good demand for vaccine and infectious diseases, ophthalmology and rare disease—all of which we are well known for,” said Adam Mendizabal, vice president and director of Emmes’ Cell and Gene Therapy Center. “But in the newer areas, then yes, cell and gene therapies continue to be area of considerable growth. What’s most significant is that we now have advanced therapies in development for nearly every single therapeutic area—from oncology through to hematology, ophthalmology, cardiology, along with neurological targets and not to mention a major focus on rare diseases. From a CRO perspective this means we need a wide breadth of clinical indications experience to build the teams for each advanced therapy trial. This is also why you will see CROs building multi-functional Centers of Excellence for cell and gene therapies so that you have these wide skill sets that can be tailored to the unique trial needs.”
Joel Morse
CEO and co-founder of Curavit Clinical Research
Finding a balance: Blending traditional and digital clinical trials for DTx
It seems to be in our nature to think of things as binary: you prefer the beach over the mountains; you like sweet treats rather than salty; this is correct and that is wrong. But such black-and-white thinking does not always serve our purpose well. Sometimes it’s simply not a zero-sum game.
When COVID-19 forced many white-collar employees to work remotely in March 2020, business leaders feared the worst. Productivity would crater, they thought, and trying to bring employees back to the office after a long absence would be impossible. Yet, those fears have mostly not come to pass because both employers and employees saw the value in moving towards hybrid work environments. Now, more than three years later, almost three quarters of US companies offer their employees a hybrid work environment that combines both in-person and remote work options. It’s the best of both worlds.
A new paradigm in clinical research
This same kind of thinking should be employed when considering clinical trials as well. Decentralised clinical trials (DCTs) gained popularity in much the same way that remote work did – out of necessity. During the pandemic, sponsors simply had no other option if they wanted to conduct a trial. And although traditional clinical trials are now available to sponsors again as COVID-19 dissipates, sponsors see the important advantages that the decentralised approach offers. So, why not combine the best of both? If office workers can do it, so can forward-thinking clinical trial sponsors.
However, to successfully embrace a hybrid approach to clinical trials, sponsors need to deeply understand their objectives, and then choose the right mix of decentralised versus in-person trial elements. If done correctly, clinical trials that are designed with digital-first principles, but which also include a strategically considered site visit component, could become the gold standard in clinical research, much the same way that hybrid work has become commonplace in a post-pandemic environment.
Nowhere is this new paradigm in clinical research more likely to become a reality than in digital therapeutics (DTx), an area of healthcare that is growing fast. While still a young sector, the DTx market is projected to grow 21.54% to reach $20 billion by 2029. Because of high incidences of chronic disease and mental health issues, along with rising demand for controlled healthcare facilities and treatment cost, demand for DTx has skyrocketed and the industry has responded by investing generously. There are now eight DTx unicorns globally.
DTx and leveraging DCTs and traditional site models
Given that DTx are software-driven and therefore can be more easily delivered to participants regardless of their location or circumstances, these products are well-suited to the decentralised trial model. And because of its flexibility, DCTs can greatly improve participant enrolment, retention, and engagement. There are no physical logistics – no shipping, storing, chain of control, cold storage, or biohazards, plus endpoints can be captured within the DTx application itself, making DCTs ideally suited for DTx studies, whether seeking regulatory approval or to bolster consumer and payer confidence. And because the DTx being studied can double as the data collection device, manufacturers often don’t need costly extra technologies like an ePRO.
Even with these advantages, DTx products can sometimes face an increased level of scrutiny in trials, and the patient screening process may require a physical engagement with a healthcare professional. Further, some DTx companies want to supplement data from the device with more traditionally collected metrics to create fuller evidence packages to meet needs of diverse stakeholders, be it regulators, payers, or doctors. As such, DTx companies see enormous value in leveraging elements of the traditional site model alongside a decentralised approach. Incorporating some in-person clinician visits can lend a greater sense of legitimacy to sceptical physicians and provide peace of mind to all.
“One of the exciting things about new technology, as well as one of the challenges, is that it really opens up new ways to develop products,” said Mike Rosenbluth, PhD, CEO at DTx company Swing Therapeutics. “Many of the processes of developing a drug are not relevant for DTx, so we’re committed to evidence development and demonstrating that our products are clinically effective – the industry needs to build on a solid foundation of evidence, so that digital therapies can be adopted as standard of care.”
Nascent therapeutics and market access complexity
Moreover, although DTx companies are producing remarkable, life-changing therapies, commercialisation has proven challenging. These nascent therapeutics often get mired in commercial processes that were originally designed for traditional therapeutics, and face market access complexity. Healthcare codes are an important part of the problem, too, for prescription and non-prescription DTx alike. These include CPT (Current Procedure Terminology) and the HCPCS (Healthcare Common Procedure Coding System). Just as product SKUs revolutionised both early supply chain management and modern e-commerce, diagnosis and billing codes are needed to unlock DTx uptake. And while a limited number exist, there is a lack of standardisation – and, manufacturers would argue, variety – to scale DTx use.
A fresh approach to clinical trials enables prescription DTx (PDTx), so as to ensure that their products can successfully navigate the regulatory process with greater ease, while also providing evidence of safety and efficacy to increase the likelihood of payer coverage, which has been a hurdle to adoption of DTx products to date (and an issue that led to the bankruptcy of Pear Therapeutics in April 2023).
“Being able to deploy and demonstrate adequate risk mitigation measures in hybrid and decentralised trials helps to assure patients, healthcare providers, and health insurers of the safety and reliability of treatment in the home or community,” explained Sabrina Taylor, PhD, CCRP, head of clinical trials at MedRhythms, a DTx company that has adopted the hybrid clinical trial model for its neurotherapeutic designs to improve walking, mobility, and related functional outcomes by using a technology platform that combines sensors, software, and music with advanced neuroscience to target neural circuitry. The company is developing a pipeline of digital therapeutics across a range of neurological conditions, including stroke, multiple sclerosis, and Parkinson’s disease. To capture safety and efficacy data across various indications, MedRhythms is leaning into the more cost-efficient DCT model and incorporating requisite in-person site visits to supplement data collection.
“One of the primary benefits of hybrid and decentralised clinical trials is their ability to increase patient access to research opportunities,” added Dr Taylor. “Plus, considering the care context serves as a useful guide when identifying the aspects of the study that must be completed in person and those that may be conducted virtually. This helps clarify the role and requirements of collaborating research sites and can be completed early in the study-planning process.”
An intersection of trial designs
Success will be achieved by the organisations that can properly identify where decentralised and traditional study designs intersect. The situation is complex, and the answer could be different even for the same patient. But, as more DTx companies begin to deploy the hybrid trial model, they will begin to find a mix of trial strategies that serve their purposes and act as roadmaps for others to follow.
“Many DTx companies develop products where the majority, if not all, of the interaction points between a company and a patient occur outside of the clinic,” Dr Taylor concluded. “Because of this, at-home data collection is a natural part of these companies’ DNA. It seems that this familiarity, combined with the cost savings, make alternative study designs a good fit for the DTx market.”
In short, find the right trial blend, and the DTx industry could revolutionise clinical trials for everyone.
Banging Down Doors to Breaking Glass Ceilings: Better Health Equity for Women
Long days and nights with only intermittent hours of sleep are not uncommon for surgical interns of any generation or gender—and such was the case in 1985 when I was doing my General Surgery internship at Strong Memorial Hospital at the University of Rochester in New York. But when I finally got my chance for a few precious hours of rest, I had to bang on doors … literally.
I was the only woman in a cohort of 20 interns, and the on-call room where we could recharge was in the back of the male doctors’ locker room. When I was on call (at least every third night), I would have to bang loudly on the male locker room door, announce my presence, and creep awkwardly along the side wall with my eyes averted, head down, to get to the door of the on-call room where I could rest. There was no female doctors’ locker room, so I would change into scrubs in the nurses’ locker room.
Fortunately, I was too exhausted to think too much about it at the time—but I was aware that, as a woman, I was battling some subtle and not-so-subtle acts of discrimination to become a surgeon.
In 1985, 2.8% of general surgeons in the US were female. Across common surgical specialties, 6.1% of neurosurgeons, 7.7% of orthopedic surgeons, 4.1% of plastic surgeons, 15.2% of ENT surgeons, 14% of ophthalmology surgeons, 2.6% of urology surgeons, 0% of thoracic surgeons, and 22.3% of OB-GYN surgeons were female.
Today, those numbers are much different: Of the 32,876 surgeons employed in the US, 48.8% are women, while 51.2% are men. And strikingly, 38% of general surgery residents in the country are women.
I completed my residency at Harvard Medical School and Massachusetts Eye and Ear Infirmary (MEEI) in 1990, graduating with all male residents, and went on to become a board-certified otolaryngologist/head and neck surgeon. I continued working at Harvard Medical School and MEEI and remained affiliated with these organizations for over 30 years. I had the pleasure of caring for thousands of patients and teaching many medical students while serving in leadership roles, including the MEEI Board of Surgeons, MEEI Pharmacy and Therapeutics Committee, and the Atrius Health Site Council.
While I broke down some doors during my clinical career, after three decades observing the problems in clinical research, I pivoted sharply. I wanted to make a broader impact on healthcare by contributing to research and working to modernize clinical trials. Joel Morse, Dave Hanaman, and I co-founded Curavit Clinical Research in October 2019 when—like the rest of the world—we had zero premonition about the pandemic yet to come that would cause clinical trial activity to grind to a halt or at least become severely limited and transformed. Our timing was uncanny.
Today, decentralized clinical trials (DCTs) continue and are moving from edge case to main case and scaling across the enterprise. According to one company’s internal analysis, average levels of decentralization in clinical trials pre-pandemic were at 43%, reaching 55% in 2022, and are expected to reach 66% within the next five years.
Catalyzed by a pandemic but evangelized by success, we are finally seeing clinical research transform.
We see a future in which more clinical trial protocols will be designed from the outset with digital-first principles that enable greater access to clinical trials among all genders, races, and demographics. This future will enable clinical research to move faster to bring more life-saving medicines to more people for less cost and enable more pharmaceutical companies to invest in rare and ultrarare disease studies because we can open trials up to people wherever they live.
I also envision a future where women are equitably represented in clinical trials across all therapeutic areas. Unfortunately, the number of female participants in research falls short today, especially in three disease areas where women are affected most: cancer, cardiovascular disease, and psychiatric disorders, where 60% of people are female, but just 42% of trial participants are female.
There is more work to do, but there is also hope for a better future with innovative technology, new operational models, and—most importantly—less bias.
It’s hard to believe that the place where I was once the only female intern graduated a class of general surgeons consisting of all women in 2017—a feat set in motion decades before. And in that time, I broke through the glass ceiling to become chief medical officer and co-founder of a start-up company, but I know I’m still in the minority … for now. Through my work and personal advocacy, I aim to end these disparities both in the male-dominated technology world and in clinical research.
But, at the very least, I will work to ensure that no woman ever again must bust through a male locker room to make it to the other side.
Twists and Turns on the Winding Road of Digital Therapeutics: From Product Development to Approval to Access
The pandemic has produced a series of seismic shifts across broad aspects of our lives, upending so much of what we had previously taken for granted. One example in healthcare is the sudden growth of digital therapeutics (DTx). DTx revenue in the U.S. is expected to reach $11.2 billion by 2030, while the global DTx market is projected to reach $56 billion in just two year (up from a forecast of $9 billion). Much of this growth can be traced back to the start of the pandemic, when the U.S. Food and Drug Administration (FDA) fast-tracked several DTx products to provide options for an increased number of patients with anxiety and depression at a time when traditional, in-person treatment methods were less available. In April 2021, too, the FDA loosened regulations surrounding approval of digital mental health tools to hasten their time to market.
Facing Challenges and Making an Impact
Today, the uses of DTx have expanded beyond mental health and their benefits are making a lasting impact across therapeutic areas, demographics, and pandemic limitations. Innovation across the DTx sector represents a critical new frontier for healthcare and an important opportunity to provide patients with a new kind of modern care. Further, as more of Generation Z enters the healthcare marketplace, these progressive approaches can expect to be welcomed with open arms. For a generation that often conducts much of its daily activity on smartphones and puts a high premium on convenience, healthcare companies that prioritize digital and embrace innovation will be more likely to see success.
Unfortunately, however, innovations relating to the commercialization of DTx have lagged those of the digital products themselves. Instead of coming to market with relative ease, many DTx have been mired in processes that were originally designed for more traditional therapeutics, such as drugs, and ill-suited for the products that are being developed by DTx companies.
“One of the exciting things about new technology as well as one of the challenges is that it really opens up new ways to develop products and then to commercialize them,” said Mike Rosenbluth, PhD, CEO at Swing Therapeutics, a DTx company founded in 2019. “The question we need to ask is how we adapt those processes for the new intervention. A lot of the processes of developing a drug are not relevant for what we’re doing in DTx.”
Thankfully, there are early signs of an evolution taking place in the development and commercialization of DTx, starting with the utilization of decentralized clinical trials (DCTs). DCTs saw a major uptick when COVID-19 struck, and sponsors had no other choice but to conduct their studies remotely. Even as pandemic restrictions lifted, the benefits of DCTs remained. For instance, hybrid and decentralized trials improve patient enrollment both in speed and in diversity by allowing sponsors to target patients without geographic limitations. Well-crafted digital engagement can reach potential participants where they regularly engage with content, capturing their interest and seamlessly bringing them into the vetting process. As a result, DCTs are often more effective at obtaining highly engaged participants that better represent the patient population than the traditional, brick-and-mortar trials.
DTx in Development
Swing Therapeutics is trialing two DTx products for the treatment of fibromyalgia, a chronic pain condition. “We’re working to expand access to clinically validated treatments to help patients when and where they need it,” explained Rosenbluth. “Right now, there are over 10 million people in the U.S. with fibromyalgia yet only about 5% have access to behavior therapies, so we are working to get this product out to all patients in need.”
Since the therapeutics being studied are digital, a decentralized trial is a natural fit. Fundamentally, a DTx is software rather than a pill or injectable, so there is no physical distribution of medicines. There are no physical logistics—no shipping, storing, chain of control, cold storage, or biohazards, plus endpoints can be captured within the DTx application itself, making DCTs ideally suited for DTx studies whether seeking regulatory approval or consumer and payer confidence. Further, because a DTx is also the data collection device, manufacturers often save costs from not needing extra technologies like an electronic patient-recorded outcome to capture data in a clinical trial. DTx trials also benefit from the many other documented advantages of a DCT, including those related to patient recruitment and enrollment.
In the Swing study, for example, the company leveraged a virtual site and was able to recruit on average 10 times the number of enrolled participants vs. those recruited from each of the study’s 22 other traditional sites that started recruiting at the same time. Without geographic restrictions, the virtual site could recruit nationwide, and the convenience of a decentralized trial incentivized more patients to enroll and participate in the comfort of their own homes, rather than in traditional clinical settings outside their comfort zone.
Concerns that the lack of face-to-face contact puts virtual sites at a disadvantage seem to be unfounded, based on the Swing study. “Actually, I would say that the [DCT patients have] been more engaged in terms of their participation than [those at] other sites in our study,” Rosenbluth said.
There is also the added benefit of reaching participants who might be new to the clinical study process, and a better representation of the population who might benefit from the new therapeutic. “In a lot of clinical trials, there is a database where you can find a narrow set of people who are active trial participants rather than someone who might be more representative of the overall population and participating for the first time,” added Rosenbluth.
Aiming for Approval and Beyond
Yet even with these positive developments, the overall processes required to commercialize DTx products remains frustrating, and gaining FDA approval, an already arduous process, is hardly the final hurdle toward achieving success. Instead, it is often just the beginning; DTx companies are then faced with a series of potentially crippling obstacles, from the battle for visibility and market access, to tackling payer- and reimbursement-related issues. Companies also face systemic institutional challenges that include steep learning curves and a lack of awareness from many healthcare providers, who often have entrenched practices about the traditional therapies that they prescribe to their patients.
A traditional pharmaceutical company might spend between $200 million and $300 million to launch a new product, bolstering it with expensive initiatives such as wide-ranging patient support programs, enormous sales and marketing teams, and comprehensive advertising strategies. For the vast majority of DTx companies, such elaborate and expensive product launches are simply not possible. As a result, innovative therapies that might have already cost millions of dollars to research and develop often never successfully reach their markets. This is an unfortunate and unnecessary failure that ultimately leaves patients with fewer options.
For DTx companies to be profitable, or even sustainable, the path to commercialization must be altered and streamlined. DTx companies can help themselves by providing strong, evidence-based data on the efficacy of their therapeutics as well as by developing innovative and less costly ways of educating and enabling physicians to prescribe digital therapeutics and get reimbursed. “We’re committed to evidence development and demonstrating that our products are clinically effective,” Rosenbluth said. “The industry needs to build on a solid foundation of evidence so that digital therapies can be adopted as standard of care.”
Paving the Way for Access
Swing’s cognitive behavioral therapy mobile application, known as Stanza, is commercially available under the FDA’s Enforcement Policy for Digital Health Devices. In addition to being available by prescription, Stanza is available through Swing Care™, an affiliated, physician-owned telemedicine clinic established by Swing Therapeutics to enable broader access to its product and place it in the context of a holistic care pathway. “We are working to find patient-centered ways to provide widespread access to our product and the holistic care patients need. We expect to expand Swing Care to more areas of the country in 2023,” concluded Rosenbluth.
The various pivots that were necessitated by the pandemic over the last few years offer a clear road map for how we can begin to take innovative approaches toward leveling the playing field of healthcare—from developing new therapeutics to ensuring equitable market access. Decentralized approaches and new technologies are the lynchpin, but require close collaboration with regulators, physicians, sponsors, payers, and patients. Without taking bold steps now, we risk potentially muting the impact of important new therapeutics and preventing critical care from reaching those who need it the most.
Joel Morse, MBA, (joel.morse@curavitclinicalresearch.com) is Founder and CEO of Curavit, a virtual contract research organization that designs and executes decentralized clinical trials. Previously, he founded C3i, a business process outsourcing healthcare provider.
“Fibromyalgia is a chronic widespread pain condition that is thought of as a central sensitization syndrome where there’s no peripheral injury that’s causing the pain but the brain is amplifying and very sensitized to pain signals,” Dr. Rosenbluth explains. “The three FDA approved medications for fibromyalgia work in a proportion of patients but they also have a lot of side effects and no new drug for fibromyalgia has made it to market since 2009. CBT is considered a first-line treatment for fibromyalgia, but people don’t tend to get it because of lack of access. So, we’re committed to changing that and getting this digital therapeutic out there.”
Increasing Access Via a Telemedicine Clinic
To help expand access of Stanza, Swing Therapeutics launched Swing Care, a telemedicine clinic focused specifically on the treatment of fibromyalgia, in October 2022. Swing Therapeutics serves as the clinic’s Management Services Organization (MSO), which is responsible for providing administrative support to the practice. However, the clinic itself is physician-owned with all medical decisions made by the practicing physicians along with its medical director, Andrea Chadwick, MD who is Associate Professor in the Department of Anesthesiology, Pain, and Perioperative Medicine at The University of Kansas Medical Center.
“Swing Care is designed to bridge the gap between patient awareness and access to Stanza when medically appropriate,” Dr. Rosenbluth says. “The clinic does digital advertising to raise patient awareness. And if they join the clinic, they can also get access to appropriate medication management to holistically treat the condition.”
Swing Care services include monthly clinician appointments, ongoing clinician messaging, and behavioral therapies. Currently, Swing Care is only available for patients in Texas, but Dr. Rosenbluth says the plan is to expand to more states in the near future.
However, Stanza is not limited to Swing Care members as the DTx can be prescribed by any physician. Dr. Rosenbluth explains that Swing Care simply offered the company a way to explore a patient access pathway to help those medically in need of Stanza get the therapy at a time when the market access landscape for DTx is still developing.
“All of the industry partners are working at it along with several senators and congress people, so hopefully that will lead to change,” Dr. Rosenbluth says. “In the meantime, there are some payers that are being more innovative such as Highmark, which has issued a positive coverage decision for some prescription digital therapeutics. There are also different business models such as directly contracting with payers or going through employer benefits.”
Embracing Decentralized Clinical Trials
As Swing Therapeutics also works toward getting full FDA approval, it has embraced another virtual solution—the decentralized clinical trial (DCT). The company partnered with Curavit Clinical Research, considered to be the world’s first ever all-virtual contract research organization (VCRO), to expand the reach of its pivotal multicenter, randomized controlled study called PROSPER-FM. The hybrid trial is expected to enroll about 270 participants recruited from 15 to 25 physical sites plus Curavit’s virtual site.
The study is comparing Stanza to an alternate digital therapeutic, a digital symptom tracker that Swing developed based on similar apps that have been validated for chronic pain management. The study will last for 12 weeks and will measure clinical endpoints through patient-reported outcomes like the Patient Global Impression of Change (PGIC) Scale and the Revised Fibromyalgia Impact Questionnaire (FIQ-R) as well as instruments that measure pain intensity and interference, sleep interference, depression, anxiety, pain acceptance, mindfulness, and quality of life.
Curavit’s virtual site and recruitment process have quickly helped to ramp up participation in the trial. Compared to physical sites that started at the same time, Curavit has enrolled 10x more patients in its virtual site. The VCRO has a lot of experience with DTx decentralized trials as more than 50% of its clients are in the space.
“We have a very rigorous process to screen and educate potential participants into this trial because a lot is expected from them,” Joel Morse, Co-Founder and CEO of Curavit, explained to PM360 in an interview. “We had to ensure that the participants are aligned with the protocol, inclusion/exclusion criteria, and that the data can be used for FDA approval. We’ve also been working with Swing to make sure that they are high-quality participants by adherence and they are doing all of the activities they’re required to do and staying in the trial. So far, we are seeing participants who at are top of the bell curve if you will.”
Curavit recruits potential participants through web advertising on Facebook, Reddit, and Twitter to build awareness of the trial. The ad directs people to a landing page that offers a combination of education about the trial as well as a self-screening questionnaire to test eligibility. If eligible, they are presented with an opportunity to have a 90-minute live engagement with a Curavit clinical research coordinator, who makes sure they are aligned with the study’s protocol and inclusion/exclusion criteria. Ultimately, this process weeds out more than 50% of the people who initially self-screened correctly.
Curavit also manages the process for patients to get their mandatory urine drug screening by lining them up with their nearest Quest Diagnostics lab and providing them with a QR code that includes payment for the session and the information for where to send the results. Once they pass through all of this, participants are scheduled to meet with the principal investigator (PI), a board-certified rheumatologist, who can ensure the patient’s diagnosis of fibromyalgia. At that stage, Curavit also works with the participant to download the application, set it all up, and make sure they know how to use it.
In a previous prospective single-arm clinical trial (REACT-FM), Swing found that 88% of participants were satisfied with Stanza and 91% preferred either using the app alone or in combination with other approved fibromyalgia medications, compared to using approved medications alone.
“At the end of the day, we’re trying to help patients change their relationship with pain,” Dr. Rosenbluth says. “The overarching idea of ACT is to help people accept what’s going on in your body and to separate your thoughts and feelings from yourself, so you can let those feelings pass. And then we’re trying to drive behavior change by helping people identify their values and taking committed action aligned with those values. It helps patients take control over their choices rather than letting their symptoms dictate their life.”
Swing Therapeutics’ Approach to the DTx Market Access Problem and Clinical Trial Recruitment
Swing Therapeutics, a digital therapeutics (DTx) company, has turned to a couple of virtual solutions to help close that last mile of commercialization that has been proving a difficult barrier for many DTx companies to cross despite a rapidly growing market. Estimates predict the DTx market to reach $11.2 billion in the U.S. by 2030 according to Nova One Advisor and $35.78 billion globally by 2030 according to Strategic Market Research, however, several DTx have failed to catch on after hitting the market due to either low awareness among doctors and patients or a market access environment that has yet to fully embrace these therapeutic options.
“Currently, Medicare doesn’t have a benefits category for digital therapeutics and that’s been a barrier,” Mike Rosenbluth, PhD, Chief Executive Officer at Swing Therapeutics, told PM360 in an interview. “Commercial payers can follow Medicare, so if there’s no standards by payers in terms of what they’ll pay for, some investors may be more cautious to invest in a sector that does not have mature business models.”
While payers may be slow to adopt DTx, that has not been the case on the regulatory side, according to Dr. Rosenbluth who says the “FDA has been very supportive of this field.” The agency has already approved nine prescription DTx, which are regulated as medical devices under the Software as a Medical Device (SaMD) program. Additionally, the FDA established the Enforcement Policy for Digital Health Devices during the COVID-19 Public Health Emergency to expand the availability of DTx options that treat things such as anxiety and depression in order to help patients at a time when they might not be able to see their doctors in person.
As part of this policy, Swing Therapeutics’ Stanza, a DTx designed to deliver behavioral therapy to people with fibromyalgia, was made commercially available to patients at the end of 2022. Previously, Stanza was granted the FDA’s Breakthrough Device Designation. The mobile app uses acceptance and commitment therapy (ACT), a form of cognitive behavioral therapy (CBT), to help improve the psychological symptoms associated with fibromyalgia, including anxiety, depression, and sleeplessness in adult patients.
“Fibromyalgia is a chronic widespread pain condition that is thought of as a central sensitization syndrome where there’s no peripheral injury that’s causing the pain but the brain is amplifying and very sensitized to pain signals,” Dr. Rosenbluth explains. “The three FDA approved medications for fibromyalgia work in a proportion of patients but they also have a lot of side effects and no new drug for fibromyalgia has made it to market since 2009. CBT is considered a first-line treatment for fibromyalgia, but people don’t tend to get it because of lack of access. So, we’re committed to changing that and getting this digital therapeutic out there.”
Increasing Access Via a Telemedicine Clinic
To help expand access of Stanza, Swing Therapeutics launched Swing Care, a telemedicine clinic focused specifically on the treatment of fibromyalgia, in October 2022. Swing Therapeutics serves as the clinic’s Management Services Organization (MSO), which is responsible for providing administrative support to the practice. However, the clinic itself is physician-owned with all medical decisions made by the practicing physicians along with its medical director, Andrea Chadwick, MD who is Associate Professor in the Department of Anesthesiology, Pain, and Perioperative Medicine at The University of Kansas Medical Center.
“Swing Care is designed to bridge the gap between patient awareness and access to Stanza when medically appropriate,” Dr. Rosenbluth says. “The clinic does digital advertising to raise patient awareness. And if they join the clinic, they can also get access to appropriate medication management to holistically treat the condition.”
Swing Care services include monthly clinician appointments, ongoing clinician messaging, and behavioral therapies. Currently, Swing Care is only available for patients in Texas, but Dr. Rosenbluth says the plan is to expand to more states in the near future.
However, Stanza is not limited to Swing Care members as the DTx can be prescribed by any physician. Dr. Rosenbluth explains that Swing Care simply offered the company a way to explore a patient access pathway to help those medically in need of Stanza get the therapy at a time when the market access landscape for DTx is still developing.
“All of the industry partners are working at it along with several senators and congress people, so hopefully that will lead to change,” Dr. Rosenbluth says. “In the meantime, there are some payers that are being more innovative such as Highmark, which has issued a positive coverage decision for some prescription digital therapeutics. There are also different business models such as directly contracting with payers or going through employer benefits.”
Embracing Decentralized Clinical Trials
As Swing Therapeutics also works toward getting full FDA approval, it has embraced another virtual solution—the decentralized clinical trial (DCT). The company partnered with Curavit Clinical Research, considered to be the world’s first ever all-virtual contract research organization (VCRO), to expand the reach of its pivotal multicenter, randomized controlled study called PROSPER-FM. The hybrid trial is expected to enroll about 270 participants recruited from 15 to 25 physical sites plus Curavit’s virtual site.
The study is comparing Stanza to an alternate digital therapeutic, a digital symptom tracker that Swing developed based on similar apps that have been validated for chronic pain management. The study will last for 12 weeks and will measure clinical endpoints through patient-reported outcomes like the Patient Global Impression of Change (PGIC) Scale and the Revised Fibromyalgia Impact Questionnaire (FIQ-R) as well as instruments that measure pain intensity and interference, sleep interference, depression, anxiety, pain acceptance, mindfulness, and quality of life.
Curavit’s virtual site and recruitment process have quickly helped to ramp up participation in the trial. Compared to physical sites that started at the same time, Curavit has enrolled 10x more patients in its virtual site. The VCRO has a lot of experience with DTx decentralized trials as more than 50% of its clients are in the space.
“We have a very rigorous process to screen and educate potential participants into this trial because a lot is expected from them,” Joel Morse, Co-Founder and CEO of Curavit, explained to PM360 in an interview. “We had to ensure that the participants are aligned with the protocol, inclusion/exclusion criteria, and that the data can be used for FDA approval. We’ve also been working with Swing to make sure that they are high-quality participants by adherence and they are doing all of the activities they’re required to do and staying in the trial. So far, we are seeing participants who at are top of the bell curve if you will.”
Curavit recruits potential participants through web advertising on Facebook, Reddit, and Twitter to build awareness of the trial. The ad directs people to a landing page that offers a combination of education about the trial as well as a self-screening questionnaire to test eligibility. If eligible, they are presented with an opportunity to have a 90-minute live engagement with a Curavit clinical research coordinator, who makes sure they are aligned with the study’s protocol and inclusion/exclusion criteria. Ultimately, this process weeds out more than 50% of the people who initially self-screened correctly.
Curavit also manages the process for patients to get their mandatory urine drug screening by lining them up with their nearest Quest Diagnostics lab and providing them with a QR code that includes payment for the session and the information for where to send the results. Once they pass through all of this, participants are scheduled to meet with the principal investigator (PI), a board-certified rheumatologist, who can ensure the patient’s diagnosis of fibromyalgia. At that stage, Curavit also works with the participant to download the application, set it all up, and make sure they know how to use it.
In a previous prospective single-arm clinical trial (REACT-FM), Swing found that 88% of participants were satisfied with Stanza and 91% preferred either using the app alone or in combination with other approved fibromyalgia medications, compared to using approved medications alone.
“At the end of the day, we’re trying to help patients change their relationship with pain,” Dr. Rosenbluth says. “The overarching idea of ACT is to help people accept what’s going on in your body and to separate your thoughts and feelings from yourself, so you can let those feelings pass. And then we’re trying to drive behavior change by helping people identify their values and taking committed action aligned with those values. It helps patients take control over their choices rather than letting their symptoms dictate their life.”
Making Clinical Trials Better for Everyone in 2023
Getting clinical trials to the finish line is not easy. Between 15% to 40% of patients, depending on the trial phase, drop out before a trial is completed, according to Atlant Clinical. And 11% of trials fail to enroll even a single patient, according to Advarra. That’s not to mention the significant diversity problem. According the FDA’s 2015-2019 Drug Trials Snapshots Summary Report, 76% of all clinical trial participants are white. So, there is plenty of room for improvement across the board to make clinical trials more accessible, diverse, and easier on patients, which starts with increasing awareness.
“Aside from the obvious trust factor that permeates throughout clinical trial recruitment, awareness is the other major contributing factor in the underrepresentation of diverse populations in clinical trials,” explains Mo Hamzeh, SVP, Management Supervisor, Ogilvy Health. “Some patients might be willing to participate if they are aware not just of the clinical trial itself but also of the benefits that come with it. This lack of awareness among patients might also be a direct reflection of the biases that investigators have when seeking patients who may be eligible to participate in clinical trials.”
One way companies can address these potential biases and increase awareness within marginalized groups is to include trusted community members in the process.
“It’s about making the neighborhood doctor a key opinion leader who can educate and inform within the community,” says David Fleishman, Chief Operations Officer, BBK Worldwide. “It’s about selecting the right location for the study site—not because there is a high patient population, but because it is an area where patients are going to be more comfortable about pursuing the care they need. And it’s about ramping up support services that address some of the common concerns that may interfere with participation, such as childcare, meal preparation, transportation, and lost wages.”
Decentralized clinical trials (DCTs), which involve utilizing technology like telehealth or remote patient monitoring as well as local healthcare services to bring trials to the patients, may also be helping in this regard.
“In a recent research project we conducted with Underscore Marketing exploring the importance of HCP-based clinical trial recruitment and critical success factors, I was encouraged to hear a repeated focus on the opportunity to use DCTs to reach both a greater number of patients and a more diverse cohort during interviews with pharmaceutical decision makers from Genentech and Otsuka,” says Christine Franklin, Executive Director, The DHC Group. “Since DCTs will produce patient claims data that will better match the real-world patient population, we are also looking forward to the resulting impact on the ability of marketers to create better and more authentic cross-cultural marketing campaigns.”
The Rise of DCTs
Patients in general are intrigued by the potential of DCTs and their ability to make participation easier on them. According to Ivor Clarke, CEO, SubjectWell, surveyed patients who were “very interested” in participation jumped from 39% to 60% when told the trial could be completed entirely at home. However, he warns that with DCTs comes a significant trade-off.
“In addition to needing reliable WiFi, a supported device, and the necessary skills to use it, patients are too often forced to navigate complex workflows on their own,” Clarke explains. “This has the potential to exclude certain demographics without sponsors and investigators realizing it. For example, SubjectWell surveyed Parkinson’s disease patients about their comfort with digital tasks and found that while 97% of patients 59 and younger were ‘very comfortable’ with a digital questionnaire, only 31% of patients 80 and older shared the same level of comfort.”
For that reason, Dr. Clare Grace, Chief Patient Officer, Parexel, says to expect a more hybrid approach to clinical trial design in 2023 that allows sponsors to meet patients where they are—both geographically and in their treatment journey.
“Every patient and trial are different, and we must recognize patients’ needs and wants to create a model that eases their participation burden,” Grace says. “This means recognizing not all patients want to participate in a fully DCT and prefer having an in-person component. Conversely, other patients may prefer participating in trials from the comfort of their own home or in their local community.”
Other Considerations for Better Trials
Patients who are skeptical of participating in trials would also like greater ownership over their data as well as the ability to continuously control access to it.
“Blockchain technologies that enable self-sovereign identity governance must be integrated into every aspect of trials, from patient recruitment and consent through to submission,” says Dave Hanaman, Co-founder, President, & Chief Commercial Officer, Curavit Clinical Research. “When patients have control of their data—not just vague ‘empowerment’ granted from a monolithic company—they will have confidence in the system because in a real sense, they will own it.”
Speaking of data, historical real-world data can also help improve the efficacy and safety of clinical trials.
“Computational disease models allow us to conduct synthetic trials on an AI platform, rather than in the clinic,” says David Harel, Co-Founder and CEO, CytoReason. “We can compare the efficacy of one drug across multiple diseases or compare multiple drugs head-to-head. The technology can help pharma and biotech companies plan their clinical trial strategies and potentially shorten trial phases, reduce development costs, and increase success rates.”
To improve patient screening and trial enrollment, Carla Balch, CEO, Spesana, says physicians crave being more involved in trial design.
Balch says, “Pharma can give physicians an opportunity to contribute intelligence by integrating collaboration into platforms designed to address the challenges physicians have identified, encouraging: 1) open discussions as inclusion/exclusion criteria is developed; 2) providing sponsors understanding of the infrastructure and standardized processes required to enable clinical trials to be as smooth a treatment process as is the standard of care; and 3) better alignment of trial criteria to more accurately represent clinical and operational behaviors inside the halls of medicine.”
Some sponsors are also using agile methodology or adaptive clinical trials to reset trial designs and parameters based on insights from the collected data.
“First developed in the software industry, agile transformation allows cross-functional teams to shift quickly,” explains Sukhwinder Kaul, Senior Manager-Clinical Insights, Axtria. “By using continuously updated analytics, sponsors or contract research organizations can refine sample size, identify sites/investigators that generate more value and focus recruiting efforts on them, and stop a trial early if it becomes clear it is unlikely to demonstrate effectiveness. Such insights can successfully define the course of a trial and shorten a product’s time to market, which is the ultimate goal of any trial.”
Why Three Doctors are in Favor of Decentralized Clinical Trials
Additionally, healthcare economists identified that despite dramatic leaps in scientific and technological advancements since 1950, drug research and development demonstrated flagging productivity in bringing new drugs to market. Retrospective analysis revealed an 80-fold decrease in drugs approved per billion US dollars spent when adjusted for inflation.
With the extensive cost and slow turnaround of traditional clinical trials, Decentralized Clinical Trials (DCTs) are gaining robust approbation as an effective, patient-centric alternative, and these three doctors will help you understand why.
Why are Traditional Clinical Trial Designs Failing Patients?
In a meta-analysis of cancer clinical trial enrollment encompassing 8,883 patients, Unger et al reported disparate enrollment in clinical trials depending on whether patients were seen in an academic (15.9%) or a community (7.0%) setting.
Regardless of setting, 55.6% of cancer patients found no traditional clinical trial available for them. Multiple stakeholders, including the National Cancer Institute (NCI), recognize the need for increased access to trials. The NCI reports that when patients are offered clinical trials, they accept 50% of the time.
But numerous barriers in recruitment for traditional clinical trials exist—among these are ease for patients to participate and time constraints on researchers. Also, unconscious bias may be introduced in patients’ clinical trial access by pragmatic considerations such as sponsor or CRO familiarity with: research sites, physician-researchers, and institution reputation.
We ask research participants—who are almost, by definition, sick—to come to participate in research studies in which they have uncertain benefit on our terms. So, [my team] started using telemedicine to bring care to Parkinson’s patients in 2007. We started doing decentralized research studies—bringing research studies to participants in 2012–2013. Research participants like it when you bring clinical research to them on their terms!
Another detriment to clinical trial participation is that they rarely include diverse populations—geographic, ethnic, and economic—from participating. In a large cohort analysis from Stanford University of all US clinical trials from 2000 until 2020, white patients were enrolled 79.7% (Interquartile range (IQR), 61.9–90.0%), compared with 10% participation by Black Americans (IQR 2.5–23.5%), and progressively lower representation of Hispanic/Latinos, Asians, and American Indians with dramatically low presence in clinical trials (0.0%, IQR 0.0-0.2%).
The Sidebar asked Dr. Pamela Diamond, Co-founder and Chief Medical Officer of CURAVIT Clinical Research—a virtual contract research organization (VCRO) that designs and executes Decentralized Clinical Trials—about what deficits she observes in traditional research models:
One deficit involves patient recruitment for traditional research trials. Generally, participants need to live close to traditional clinical research sites, and that can make it difficult to recruit and retain participants. Also, traditional clinical trials often fail to recruit participants who belong to racial and/or ethnic minorities. When diverse groups aren’t part of a study, we can’t be sure that the treatment will work in all populations, and we can’t predict whether side effects might emerge in one group or another.
Another deficit that comes to mind pertains to rare disease research. If there are very few people in the country that have the rare disease being studied, it’s very challenging to bring those participants into traditional brick-and-mortar research sites. Rare disease research is certainly one area where DCTs can play a very important role.
Decentralized Clinical Trials can Enhance Patients’ Access to Investigational Therapeutics
Traditional clinical trials can take as long as 12 years to develop a new therapy, recounts Dr. Michelle Longmire, CEO of Medable, a privately owned, venture-backed Decentralized Clinical Trial Platform that designs and digitally streamlines DCTs.
Dr. Longmire is a former Stanford University School of Medicine academic dermatologist with extensive experience in traditional clinical trials researching systemic sclerosis, a life-threatening dermatologic condition. The Sidebar asked Dr. Longmire what frustrations with traditional clinical trial designs inspired her to found Medable:
Caring for patients, as a physician-scientist, you have this incredible satisfaction in seeing patients every day. You are front and center with patients’ conditions that they live with. In my work with Systemic Sclerosis (SSc), this condition had a 90% mortality rate, prior to discovering sildenafil as a treatment for the lung manifestations of SSc.
With traditional trial designs, you see how slow the process is, and how much patients need to be able to see change faster, in terms of therapeutics available to them.
So, what I observed was just the overarching challenge of ‘How do we develop drugs faster?’. I saw a huge opportunity to enable better access to people to allow them to be part of that clinical development process that could make this process faster… So, let’s broaden access! Let’s make it so everyone living with this condition can have the opportunity to benefit from these investigational drugs. And, ideally, make that drug development process faster by virtue of allowing more patients to participate.
The Pandemic Enters, Stage Left
The 2020 global SARS-CoV-2 pandemic accelerated political, regulatory, and public acceptance of the role of digital therapeutics in providing high quality medical care. Most evidently, the near halt of ongoing traditional clinical trials highlighted the critical need for creative, progressive research designs that offer patients access to therapeutics for life-threatening and chronic diseases.
Starting up CURAVIT Clinical Research during the COVID-19 pandemic presented many challenges, but, in a lot of ways, the pandemic accelerated the growth of our company. There were many site-based trials that came to a screeching halt in early 2020. Participants could not get into the sites for their assessments. In many ways, the challenges of the pandemic made sponsors, research groups, CROs (contract research organizations), and participants more open-minded about becoming involved in Decentralized Clinical Trials.
Intuitively, DCTs are patient centric. However, while acknowledging the benefits of trial modifications, regulatory agencies and industry stakeholders strive to provide evidence of DCT efficacy, both clinically and economically.
What’s the Evidence Supporting DCTs?
A 2022 Tufts Center for the Study of Drug Development (CSDD) Impact Analysis showed that using DCT methods in Phase II studies provided a five-fold ($8.6 million) return on investment (ROI), and a 13x ROI for Phase III drugs ($40.1 million dollars) per investigational drug. This was based on an independent analysis of DCTs from Medable.
Tufts CSDD analysis concluded that the largest benefit results from reductions in cycle time moving from Phase II to Phase III clinical trials.
Analyzing industry confidence in DCTs, McKinsey & Company reported that in 2020, 100% of pharma and CRO participants surveyed responded they expected virtual trials to be a major component of their portfolios. And 89% anticipate their company running home-based clinical trials with participants—representing a dramatic increase in endorsement of DCTs from 2019.
Are Regulatory Agencies ‘On Board’?
Regulatory agencies recognize that traditional clinical trials are expensive. In a 2018 study, Johns Hopkins researchers identified that clinical trial costs can range from $2 million dollars to $347 million dollars. The number of participants, length of the trial, and the ability to meaningfully influence clinical outcomes of the targeted disease can increase costs significantly.
The Sidebar asked Dr. Michelle Longmire, CEO of Medable, why the medical research and pharma communities were slow in embracing DCTs—until now. Dr. Longmire explains:
The stakes are high. You have patients’ lives on the line, and an expensive process, close to 3 billion dollars, according to Tufts. I think that it’s hard for people to deviate from the status quo unless they must.
We didn’t get meaningful adoption of DCTs until the pandemic, when we actually had to get people to do it differently because the sites were closed. The status quo is all that people are willing to go with until there is something that forces them to change.
In a 2021 meeting of the directors for NCI-designated cancer centers, FDA regulators demonstrated enthusiasm and embracement of DCTs. In addition to predictable benefits like improved recruitment, they identified these benefits of DCTs:
• Data capture outside of the healthcare setting.
• Continuous data rather than snapshots.
• Objective measurements.
• Reduced missing data.
• Capturing rare events.
Recognizing the advancement of DCTs, the FDA’s Oncology Center of Excellence is now evaluating how modifications made to oncology clinical trials, during the COVID-19 pandemic, can be assessed for quality of evidence and future trial guidance.
The Sidebar queried Dr. Pamela Diamond, Chief Medical Officer of CURAVIT, on her experience regarding the FDAs’ uptake of DCTs. She noted:
An impetus was the COVID-19 response. In late 2021 and early 2022, the FDA published guidelines on DCTs: services and on the use of digital health products in trials. Those guidelines have been very helpful.
I think it is good advice to sponsors, CROs–anyone designing and executing DCTs–to consult the FDA early and often. It’s helpful to get the input of the FDA about the protocol design and product-specific questions, garnering the FDAs advice on the selection of technology that might be used in conducting the research trial.
Are the Central Stakeholders Ready to Pivot?
DCTs can’t progress without their two main stakeholders embracing the transition: patients and clinician-researchers. In 2021, Labcorp™sponsored a survey of US and UK oncology clinician researchers’ and patients’ perceptions of DCTs. The by oncologists revealed they were reticent about possible decreased oversight, increased patient responsibility, and quality of samples.
Patients, on the other hand, revealed their general concerns were related to the potential for side effects to occur, distance from the hospital, or not receiving the therapeutic drug (receiving a placebo). Confirming The Sidebar’s observations, of the patients surveyed, 90% revealed they would not travel over 10 to 50 miles to participate in a research study.
Regarding exclusions to patient participation in research, Dr. Ray Dorsey, Professor of Medicine at the University of Rochester recounts his philosophy:
We have cared for patients in 5 states, and 6 continents. Since 2007, we have performed at least a dozen decentralized studies involving thousands of individuals with and without Parkinson’s disease and other conditions over the last ten years.
How do we do that? We don’t do that by embracing the status quo. We do that by developing new approaches that leverage technology to bring care to patients and research opportunities to participants. When we do that, we get a more equitable system, better health, and better knowledge that can fuel better treatments!
DCTs: Broadening Access, Enhancing Equity
Clinician-researchers and patient advocacy groups recognize the challenges and limitations of traditional clinical trials, which has inadvertently excluded patients in diverse socioeconomic and cultural strata. The onset of the COVID-19 pandemic pushed industry stakeholders, researchers, and patients to view clinical trial participation in a new light.
These broadened perspectives are buoyed by increased clinician support and patient acceptance for digital therapeutics’ role in supporting healthcare and DCTs. With increasingly creative DCT designs, even patients with limited digital access have the opportunity to participate in emerging treatments. DCTs are now ‘center stage’ in effecting clinical trials—facilitating rapid progress in crucial drug development, enhancing diversity and interpretability of trial results, and enhancing equity in patient access.
In Part II of our series, Natural Allies: Decentralized Clinical Trials and Digital Therapeutics, we will explore how DTx and DCTs are inter-reliant, augmenting patient participation in the worlds’ best investigational solutions.
Digital therapeutics 2023: Swing and trial partner Curavit kick off fibromyalgia study
After the boom-and-bust cycling in digital therapeutics over the past few years, digital health providers are looking for 2023 to be a stabilizing year. Two of those companies are digital therapeutics developer Swing Therapeutics and all-virtual CRO Curavit Clinical Research.
The pair are currently enrolling a trial for Swing’s Stanza, a prescription smartphone DTx for fibromyalgia. The cognitive behavioral therapy treatment, which received a breakthrough device designation from the FDA in 2021, became available for patients in September, alongside the formal clinical trial which will finish enrollment soon with the study set to complete in the third quarter.
“This is the first of multiple digital therapeutics for us. We’re targeting other chronic pain conditions that can be related to fibromyalgia – central sensitization syndromes is what they’re called,” Swing Therapeutics CEO Mike Rosenbluth said in an interview.
Swing is taking a different approach in digital therapeutics to help advance adoption. It’s developed an affiliated physician-owned telemedicine clinic, Swing Care, to “bridge the gap between patient awareness and access to Stanza,” Rosenbluth said.
For Swing, instead of creating a big salesforce to go out and educate physicians, patients can access Stanza, if appropriate, directly through the dedicated clinic, he said.
Another innovation is its use of virtual clinical trials through Curavit. Swing is Curavit’s tenth digital therapeutics client in fewer than six months, said Joel Morse, Curavit co-founder and CEO, with DTx companies making up about half of its client base.
Curavit has engineered a way for patients to never have to go to physical sites. While the Swing fibromyalgia study participants do have an option to participate in-person and digitally, the Curavit enrollees join the trial and engage with study coordinators and investigators entirely through telehealth.
Rosenbluth said Swing did have questions about running trials remotely and an initial concern that engagement might not be as high with patients never having to show up somewhere. That hasn’t been the case, though.
“Patients participating from Curavit’s site are just as engaged or even more so than the average patient in our studies in terms of compliance, patient reported outcomes and with the digital therapeutic itself,” he said.
Virtual Site Brings Speed, Diversity, And Engagement To Digital Therapeutic Trial
Digital therapeutics (DTx) are a natural fit with the decentralized clinical trial (DCT) model and the COVID-19 pandemic has been a major driver of demand for both. The hybrid-designed PROSPER-FM trial is a good case in point. The devices being studied are a digital Acceptance and Commitment Therapy (ACT) program and digital symptom tracker for adults with fibromyalgia, a surprisingly common and chronic affliction, and the single virtual site, run by Curavit, has been enrolling 10 times more patients than all other bricks-and-mortar sites starting at the same time.
That’s what’s being reported in a status update on the trial by Mike Rosenbluth, Ph.D., CEO of sponsor Swing Therapeutics and Joel Morse, cofounder CEO of Curavit, the world’s first all-virtual contract research organization (CRO). They agree that inclusion of the virtual site is proving to be a great way to broaden access to the study and enhance diversity while improving participant engagement overall.
The hybrid approach was a “smart strategy” by Swing, allowing the startup to balance the risk of betting on the wrong distribution channel before the evidence was in, says Morse. The virtual approach is still new and, understandably, the industry wants to see the data demonstrating its efficacy.
It’s looking good so far, says Rosenbluth, and not just in terms of enrollment. Participants are also staying in the trial and adhering to the protocol. The risk going in was that patients enrolled remotely could be less engaged and thus less likely to know, and do, what they’re supposed to. That the opposite has happened has been “really interesting.”
The enrollees recruited remotely include notoriously hard-to-reach populations, notably Native Americans located nowhere near a physical site, Morse says. Part of the trick is doing the upfront work of making the entire process virtual so individuals can truly participate in the trial from the comfort of their home.
Curavit, like Swing Therapeutics, is a young company. It was founded in early 2020—right before COVID-19 was declared a pandemic—to focus on DCTs, says Morse. Previously, he founded a company called C3i (sold to Merck in 2014 and subsequently purchased by HCL Technologies Limited) that grew into a $100 million global firm that split its time on global clinical trial execution and pharmaceutical commercial services.
That gave Morse 15 years of experience building out the service offering of Quintiles (now IQVIA), then C3i’s biggest client, as well as all of Medidata’s tier 1 and some of their tier 2 global core services. During this period, he also had plenty of practice running global clinical trials for sponsor companies big and small.
After getting his Ph.D. in biomedical engineering, Rosenbluth blazed his career path in early-stage venture investing with a focus on startup medical device and biopharma companies. Swing’s acting chief medical officer was also responsible for the last drug (milnacipran) approved for fibromyalgia in 2009, he notes.
Stanza, the prescription digital therapy app designed to deliver behavioral therapy to people with fibromyalgia, is the lead product of Swing Therapeutics, founded in 2019. But the company is also exploring other therapeutic areas, including several autoimmune diseases, where digital therapeutics can make a difference.
Scaling Treatment
The prescription DTx under investigation in the PROSPER-FM trial provides an innovative form of behavioral and cognitive therapy that is a first-line treatment for fibromyalgia, a widespread pain condition affecting 10 million people in the U.S. In addition to chronic pain, afflicted individuals can suffer from a host of comorbidities such as disturbed sleep, difficulty concentrating, and mental health impacts that include depression and anxiety, explains Rosenbluth.
Three drugs for treating fibromyalgia have been approved by the U.S. Food and Drug Administration (FDA): pregabalin (Lyrica, Pfizer), duloxetine HCL (Cymbalta, Eli Lilly), and milnacipran (Savella, Forest Labs/Cypress Bioscience). Prescription drug therapies have widely varying degrees of effectiveness but, even if they work, many patients opt to stop taking these drugs within a year because of intolerable side effects, Rosenbluth says.
In a public meeting with the FDA, patients reported that non-pharmacological approaches proved more reliably effective. Cognitive behavioral therapy with ACT—the aim of which is to help people accept their feelings as they are and commit to taking useful action in line with their personal values—has also been scientifically demonstrated to have positive effects on pain-related functioning, mental health-related quality of life, self-efficacy, depression, and anxiety (European Journal of Pain, DOI: 10.1002/j.1532-2149.2012.00224.x)
Scaling this “very specialized treatment” to accommodate the large population of patients with the disease has been the main challenge, says Rosenbluth. Swing’s answer was to develop a smartphone-based application to deliver the treatment digitally. And it received a Breakthrough Device designation from the FDA in hopes of more quickly bringing the product to market by creating an open, ongoing dialogue with the agency to ensure the evidence being built with the PROSPER-FM trial aligns with regulatory expectations of a submission package.
Prescription DTx are regulated as medical devices under the FDA’s Software as a Medical Device program, Rosenbluth says. Nine such devices have been approved to date.
Protocol Reengineering
The 12-week PROSPER-FM study started in February 2022 with 25 physical sites and a goal of enrolling up to 300 participants, says Rosenbluth. Participation requires six patient visits, and the primary endpoint is patient global impression of change per electronic patient-reported outcomes.
The study is expected to finish enrollment in the first quarter of 2023, Rosenbluth continues. Curavit was added to the mix in August with the expectation that its digital outreach approach would expand access to a broader patient population than would typically participate in clinical research by virtue of geography.
Adding a virtual site required making a few adjustments to the study workflow, says Morse. This most notably included reengineering of the one-step screening process requiring a urine drug screen and confirmation by the principal investigator (rheumatologist) that a would-be participant has fibromyalgia. For remote participants, the three-step procedure is for clinical research coordinators to conduct a 90-minute telehealth visit to screen individuals (eliminating half of the pool of prospects), who then go to a nearby drug center with a QR code to get a urine drug screen and subsequently have a televisit with the rheumatologist (again cutting the patient pool by 50%).
The changes were necessary for the virtual part of the trial to work to ensure appropriate individuals were enrolled as well as remove unnecessary burdens on patients, Morse says. Other than better reaching several underserved populations, he adds, people enrolled remotely looked very similar to those enrolled by the bricks-and-mortar sites. But, overall, they interacted more with the virtual site than their counterparts enrolled at a traditional research site.
While the virtual site has certainly augmented enrollment, the bricks-and-mortar locations are likewise indispensable when it comes to ensuring diversity, Rosenbluth says. “We are also relying on sites that are very experienced in conducting fibromyalgia studies and can help all the sites as they learn from each other, and Curavit has been able to take advantage of some of those learnings, too.”
From the FDA’s standpoint, a chief concern with remotely enrolling participants is identify verification, which represented a protocol amendment, says Rosenbluth. But, broadly speaking, the agency views DCTs favorably due to its interest in equitably expanding trial access.
The DTx industry, through regulatory guidelines and with the support of the Digital Therapeutics Alliance, is “working hard” to ensure its collective voice is heard with the FDA, Morse adds. “Frankly, regulators have been very open to hearing that voice and partnering… for the good of everyone.”
It’s a group that would be difficult to ignore. The global DTx market, valued at $42 billion in 2021, is projected to reach $56 billion over the next five years with an estimated compound annual growth rate of 26.1%.
In the U.S., the DTx market is expected to hit $11.2 billion by 2030. One of the drivers has been the FDA’s pandemic-related fast-tracking of commercial availability for prescription DTx products for treating patients with psychiatric conditions under the agency’s Enforcement Policy for Digital Health Devices during the COVID-19 Public Health Emergency, says Rosenbluth.
Gaining Traction
Digital therapeutics have many advantages—notably, no issues with shipping, storage, chain of control, cold storage, or biohazards, plus endpoints can often be captured within the DTx application itself. Yet DTx products face challenges including lack of physician awareness and the inability of doctors to easily prescribe them to patients, says Rosenbluth.
The questions looming large are how to convince physicians to prescribe a technology they’re unaccustomed to, and how to get payers on board so the device is a reimbursable expense. At Swing, the answer was to establish Swing Care, an independent online virtual medical practice devoted to the holistic treatment of fibromyalgia patients that is now operating in Texas and will expand to other states over the next year.
Clinics can prescribe traditional medications as well as digital therapeutics, Rosenbluth points out. Stanza is currently commercially available, ahead of marketing clearance, under the FDA’s Enforcement Policy for Digital Health Devices during the COVID-19 Public Health Emergency.
The parallel in the PROSPER-FM trial, he says, is the use of the 25 sites to distribute digital therapeutics to patients. In lieu of relying on a traditional CRO, Swing Therapeutics is working directly with those sites to remedy any issues they encounter and better understand the patient experience.
“Patient compliance is really important,” adds Rosenbluth, which is about keeping individuals engaged and supporting them through the study process (e.g., text message reminders). Swing has also learned from Curavit the value of digital recruitment campaigns, such as targeted ads on Facebook, Reddit, and Twitter, and plans to implement those approaches on the commercial side of the business.
Top industry experts weigh in on what the new year holds for the pharma industry.
PREDICTION #1: In 2023, the chasm will widen between those companies investing in analytics-based, digital-first commercial models and those still sitting on the fence and taking a measured approach
Alan Kalton
Life sciences companies are notoriously cautious. However, COVID-19 put many companies in the uncomfortable position of forcing new ways of working, engaging with customers, and new technologies. For many companies, the changes are sticking, ushering in the digital-first era.
We have started seeing the impact of the adoption of new technologies, such as platform intelligence solutions, ‘on the ground.’ In fact, 89% of companies surveyed by DHC Group reported that they are successfully executing an AI-driven omnichannel strategy across sales and marketing and scaling up.1
Gone are the days when digital and analytics technologies were merely a shiny new toy to test-run in isolated markets. Today, many companies understand the impact of AI and recognize that it needs to be powering engagement across all markets. As the global director of field force AI enablement at Novartis noted recently during our Omnichannel AI Masterclass, “in three to five years, I hope that our industry has moved to where AI isn’t a buzzword, but rather, it’s baked into the mainstream of our go-to-market strategies because it’s so essential.”
The organizations delaying investment in scaling intelligence platforms across the organization will see a widening gap between them and their competitors in terms of influence, customer engagement and ultimately, financial success.
Alan Kalton, Global SVP
Aktana
PREDICTION #2: Companies will connect data science models to day-to-day operational activities to execute on strategic business goals across the entire organization
David Ehrlich
Next year, we will see the start of the next chapter in AI for life sciences commercial organizations.
Traditionally, AI has lived in one of two places–either with headquarters teams, analyzing massive amounts of data to generate ‘smart’ conclusions, or within discrete applications, helping to tune the application’s impact (i.e. marketing automation systems). At headquarters, AI is used to strategically assess business opportunities on a broad scope whereas the tactical AI embedded into individual applications is very specific and application limited.
Both are valuable, but what’s missing is the connective tissue between HQ’s broad-scope AI to the various operational systems required to execute HQ’s strategic business goals. Such connective capability would reach into the multiple operational systems required for execution and guide the appropriate actions. As a result, operating teams could agilely deploy data science models to guide a wide range of day-to-day activities.
Ultimately, companies will be both more effective (more good decisions) and more efficient (less bad decisions that waste resources), cycling through the “try it, fix it” rhythm much faster to continuously improve AI’s outputs across the entire organization.
David Ehrlich, CEO & Chairman
Aktana
PREDICTION #3: AI-driven identification of digital opinion leaders (DOLs) will accelerate evidence dissemination
Deepak Patil
Medical Affairs teams are racing to provide a personalized “Netflix-like” engagement for ever-expanding targets, predicting needs and preferences and then delivering unbiased scientific information in the most useful formats and channels. Field medical affairs or medical science liaisons (MSLs), work to engage with physician key opinion leaders (KOLs), but also have a new target: digital opinion leaders.
DOLs, in essence, are KOLs active on digital platforms. DOLs may be practicing or non-practicing HCPs but have major influence over consumer behavior and informing other physicians. Some rise to near-celebrity status, such as Dr. Mikhail Varshavski–better known as Dr. Mike–who has a combined social media following of over 21 million people. He has been featured in Time, Men’s Health, Business Insider, and People Magazine, to name a few. Also, Dr. Don Dizon is a professor at Brown University and director of medical oncology at Rhode Island Hospital who shares cancer research via video primarily on TikTok. He has 38,000 followers.
In addition to doctors, nearly 90% of all adults in the U.S. search for health information on Facebook, Twitter, YouTube, and other social media sites. From doctors to patients, MSLs can multiply their influence by engaging with the right DOLs. AI and natural language processing technologies can help by mining available information–based on specialty, therapeutic area expertise, followers, outreach network, and posts–to help identify the right influencers to engage and cultivate a relationship.
Next year, as the role of the MSL continues to expand and evolve, MSLs will demand new smart technologies to help them engage with the growing fleet of digital influencers. And when these relationships are formed, MSLs will increase education and information dissemination faster and farther than they have ever done before.
Deepak Patil, Senior Director of Medical Strategy
Aktana
PREDICTION #4: Decentralized clinical trial market will continue to grow, even in economic downturn
Joel Morse
Industry leaders are debating whether or not decentralized clinical trials (DCTs) will become the norm rather than the exception across therapeutic areas–but, it’s neither. In 2023, the question will no longer be an “either/or” scenario. There will always be some trials and some elements of a trial that should not be decentralized. In 2023, however, the first question all sponsors will consider at the start of protocol design will be “what aspects of the trial can be decentralized.”
For some trials, the answer may be “all of them,” and for other trials, such as highly complex oncology trials, the answer may be “very few of them” as each trial has unique needs. However, with the rapid maturation of digital technologies and increasing comfort level with digital tools by patients and doctors, sponsors will adopt a digital-first mindset for every trial.
Digital technologies will be considered from the start rather than force-fitting them into a trial mid-way, which will ensure a more successful trial design overall. The financial and time savings of the DCT model, coupled with the remarkable patient benefits of greater access, increased convenience, and optionality, are too compelling for sponsors not to lead with it for each trial they invest in.
Joel Morse, Co-Founder & CEO
Curavit Clinical Research
PREDICTION #5: Digital therapeutics companies will focus on the difficult last mile to commercialization
Dave Hanaman
Historically, digital therapeutics (DTx) companies have directed about 95% of their effort into gaining FDA approval and 5% into market access strategy. In 2023, this will shift to a 60%/40% split, with DTX companies having an earlier focus on the commercialization process, while simultaneously working toward earning FDA approval.
This ‘last mile’ is completely unchartered territory for DTx companies.They face new obstacles bringing their therapeutics to market. For example, physicians’ lack of awareness of the DTx and their inability to easily prescribe them. There are still many unknowns around getting DTx products on the formulary and how to prescribe them to patients–doctors can’t just write a prescription and send patients off to the local drugstore when prescribing the use of an app.
And, whereas traditional drug companies may spend up to $300 million to launch a product, most DTx startups don’t have the budget to spend on commercialization strategies such as building a field team, equipping marketing teams with supporting analytics technology, and initiating patient support programs to help patients learn to use these software-based therapeutics.
Dave Hanaman, Co-Founder & Chief Commercial Officer
Curavit Clinical Research
PREDICTION #6: Clinical trial sponsors will drive a new framework for DCT technology and services (rather than the other way around)
Even with nearly nine in 10 sponsors saying they will use some elements of DCT technologies in their trials, we still have a lot to learn. We’ll continue to see a lot of experimentation in trying to understand the most effective new methods, technologies, and processes for designing and executing DCTs and improving various aspects of clinical research. But, with business models in flux and an uncertain economy, we’ll see more disruption in the DCT software space, as technology providers pivot to meet industry needs.
For instance, technology providers will work to resolve the complexities of DCT software integration, and drill down to solve specific trial problems rather than offer ‘end all be all’ solutions to sponsors that prefer a hybrid approach. Until recently, the progress of DCTs has been largely driven by providers – often, working in a bubble without collaborating closely with trial sponsors.
In 2023, sponsors will take the lead. Rather than technology providers dictating what their product/services can do to improve clinical research, sponsors will seek technology providers that solve their specific challenges. As they become more researched and familiar with DCT technologies, sponsors will define what trial improvements are required, and successful technology manufacturers will pivot accordingly.
Joel Morse, Co-Founder & CEO
Curavit Clinical Research
PREDICTION #7: Next year, decentralized and hybrid clinical trials will become simply “clinical trials”
Sanskriti Thakur
The decentralized clinical trial (DCT) model works and works well. It’s no longer a leap of faith, as a 2022 study from the Tufts Center for the Study of Drug Development shows that DCTs can achieve net financial benefits ranging from five to 13 times for Phase II and Phase III trials, equating to roughly $10 million and $39 million ROI, respectively. COVID-19 made DCTs a necessity. Positive returns will make DCTs the de-facto standard.
Expect 2023 to be a pivotal year, capping a year or more of strong growth2 in decentralized and hybrid clinical trial deployment. The next evolution of DCTs will involve self-service tools that enable sponsors and sites to deploy and operate global studies on a common platform using standardized processes. We see evidence of this pivot from customers and partners who aim to leverage digital tools across their pipeline. The industry is no longer dipping their toes in the DCT water; rather, leading pharmaceutical companies like GSK and AstraZeneca, are expanding its use.2, 3
We are living the evolution of clinical trials – similar to how consumers migrated to online banking without even realizing that a major shift was taking place in their everyday lives. Sponsors, sites, and patients will expect digital tools to drive clinical trial performance, superior experience, greater diversity, and better outcomes.
Sanskriti Thakur, Chief Growth Officer
Medable
Sources:
The DHC Group, “The State of Omnichannel HCP Engagement in Pharma,” (November 2022).
The life sciences industry is flexing towards innovation in new areas, faster than ever before, and increasing patient care in astonishing ways. Decentralised oncology trials, for example, have shown actual predictive outcome value. We can now measure patient activity, steps, and movement continuously and in real time, which serves as a new potential indicator of treatment effectiveness.1 And, digital therapeutics have emerged as an effective treatment for chronic diseases, including mental illness. The rapid innovation is both exciting and disruptive, so it’s important to strategise accurately for what we can expect in the year ahead.
Prediction 1: the FDA will become more directive and collaborative on guidelines for DCTs.
Traditional protocol designs are built upon years of empirical evidence and consensus among highly rated peer reviewed journals. For new decentralised approaches, this is practically non-existent. This will lead to more pre-protocol design discussions between sponsors and CROs and regulatory bodies seeking input on new and potentially acceptable approaches to, for example, measure digital endpoints. The risk of not having these discussions is to conduct expensive trials only to discover too late that they were measuring the wrong endpoint, in the wrong way, or with a tool or technology the FDA does not accept.
Curavit is currently conducting a decentralised trial for a digital therapeutic that began with discussions with the FDA. In this case, the indication was well-known, treated for decades by traditional medical interventions, and copious peer reviewed data to call upon. However, since the route of administration itself was new – i.e., digital rather than in pill form – all stakeholders recognised how crucial it would be to involve the FDA early and often. Specifically, they discussed which patient survey format would be best, which scores to include or exclude, and acceptable means of data capture.
As this collective body of experience continues to proliferate, 2023 will see additional FDA guidance. It is likely that the FDA will address various elements associated with DCTs more granularly than ever. These may include best practices for measuring digital endpoints, biomarkers, and telemedicine and ePRO (Patient Reported Outcomes), as well as risk factors most concerning to the FDA. For instance, at a recent presentation to the Society of Quality Assurance 2022 Annual Meeting, the FDA Office of Regulatory Affairs Bioresearch Monitoring Division Director Anne Johnson emphasised that DCTs are largely reliant on electronic data integrity and therefore subject to firmly established 21 CFR Part 11 compliance.2
Prediction 2: More clinical trial services will become remote, beyond just patient monitoring.
We will see continued increases in remote clinical trial activities and services in 2023, such as remote monitoring, remote site staff training, remote site activation visits, remote quality management meetings, remote safety management meeting,s and more.
These unprecedented clinical trial activities represent a fundamental shift that is still unfolding. There was a time when Source Data Verification (SDV) by any other means than frequent and extremely costly on-site CRA visits was unthinkable. We now see continuing proof points that conducting SDV remotely can not only save time and travel costs, but can also increase quality.
Curavit recently worked on a 28-site, US-based trial where more than half of the source data verification was conducted remotely with secure, remote access to the eTMF and EDC systems. Instead of using generalised, on-site CRAs, Curavit’s therapeutic area specialists handled this significant task from afar, prioritising specific expertise over physical proximity. This had a significant impact on data quality and speed, as well as reductions in travel and costs. Curavit was also able to conduct additional Q/C measures simultaneously, which otherwise would have been a separate process.
Prediction 3: AI innovation will expand its application to enhance patient experience.
Although “Enquire Here” buttons are common for large patient enrolment providers, recent advances in Natural Language Processing (NLP) – a form of artificial intelligence or AI – allow for far greater, more meaningful, and effective patient engagement. Technologies such as BERT3 and GPT-3 catapult NLP capabilities beyond basic processing, into the realm of language intelligence. Potential applications will surpass current-day screening chat bots, which automate FAQ workflow and are only capable of answering the most basic patient questions.
In 2023, expect to see AI innovations improve enrolment agility and, most importantly, the patient experience in a clinical trial. For instance, NLP will respond to patient concerns or enquiries with more humanised responses and alert clinicians faster and automatically. This will, in turn, improve patient interest, trust, engagement, enrolment, and clinical trial retention. In addition to patient benefits, AI will enable actionable real-time metrics and analysis and a near-immediate feedback loop on the investigational drug’s impact on patients’ daily lives.
Prediction 4: digital therapeutics companies will focus on the difficult last mile to commercialisation.
Historically, digital therapeutics (DTx) companies have directed about 95% of their effort into gaining FDA approval and 5% into market access strategy. In 2023, this will shift to a 60%/40% split, with DTx companies having an earlier focus on the commercialisation process, while simultaneously working toward earning FDA approval.
This ’last mile’ is completely unchartered territory for DTx companies. They face new obstacles bringing their therapeutics to market – for example, physicians’ lack of awareness of the DTx and their inability to easily prescribe them. There are still many unknowns around getting DTx products on the formulary and how to prescribe them to patients – doctors can’t just write a prescription and send patients off to the local drugstore when prescribing the use of an app.
And, whereas traditional drug companies may spend up to $300 million to launch a product, most DTx startups don’t have the budget to spend on commercialisation strategies such as building a field team, equipping marketing teams with supporting analytics technology, and initiating patient support programs to help patients learn to use these software-based therapeutics.
Beyond 2023 – the Sovereign Patient ID
The concept of patients owning their own data has been around since the advent of electronic health records. However, 2023 will see new technologies such as blockchain and smart contracts bring the Sovereign Patient ID concept closer to reality. This will give the patient the ability to own their own identity and associated data on their own devices, as opposed to their identity being created and stored separately by each service provider: a state of error prone, redundant inefficiency. The life sciences industry will collaborate and share lessons learned with other verticals that are currently exploring the same concept, such as “Self-Sovereign Identity” (SSI).4
This problem will not be solved in 2023, but progress will be made.
References
1. Gresham G, Hendifar AE, Spiegel B, Neeman E, Tuli R, Rimel BJ, Figlin RA, Meinert CL, Piantadosi S, Shinde AM. Wearable activity monitors to assess performance status and predict clinical outcomes in advanced cancer patients. NPJ Digit Med. 2018 Jul 5;1:27. doi: 10.1038/s41746-018-0032-6. PMID: 31304309; PMCID: PMC6550281.
2. Chapman, J. An FDA Perspective on Decentralized Clinical Trials: Part 1. July 28, 2022.
3. Devlin, J, Chang, M.W. Open Sourcing BERT: State of the Art Pre-Training for Natural Language Processing. November 2, 2018.
4. Preukschat, A., Reed, D. Self-Sovereign Identity- Decentralized Digital Identity and Verifiable Credentials. Manning. 2021.
About the Author
Dr. Pam Diamond is co-founder and chief medical officer of Curavit, a virtual contract research organisation (VCRO) that designs and executes decentralised clinical trials. She is a board-certified, Boston-based otolaryngologist/head and neck surgeon who was affiliated with Harvard Medical School (HMS) and Massachusetts Eye and Ear Infirmary (MEEI) for over 30 years. At Curavit, Dr. Diamond provides medical and scientific expertise and oversight to the design and execution of Curavit’s decentralised clinical trials. She received her medical degree from the University of Rochester School of Medicine and completed her otolaryngology/head and neck surgery residency at Harvard Medical School/MEEI.
Digital Therapeutics: From Product Development and Approval to Commercialization and Reimbursement
Estimates of the US digital therapeutics (DTx) market have jumped by billions each year since 2019 and, as of November 2022, is expected to hit $11.2 billion by 2030, while the global DTx market is projected to reach $56 billion over the next five years. The market was driven by the FDA fast-tracking pandemic-related approvals for prescription DTx products to help treat the sharp increase in patients with anxiety and depression.
There are many types of DTx manufacturers, ranging from emerging DTx companies to public companies like Pear Therapeutics and Akili Interactive to global pharmaceutical companies like Roche and AstraZeneca, which are acquiring or partnering with DTx startups to enter the market.
To add further complexity, there are FDA-approved prescription digital therapeutics, nonprescription digital therapeutics, and those that may eventually seek approval.
Benefits of digital therapeutics for trial recruitment
Traditional clinical trials are complex, but architecting a DCT from the ground up is even more complicated. And while nearly nine in 10 sponsors say they use some elements of DCT technologies in their trials, fully virtual trials are still rare. At a recent conference, one top-10 pharma executive said that while more than half of their trial site visits are virtual, no trials are 100 percent virtual.
One reason for this is because designing a DCT protocol requires highly specialized expertise. Sponsors are leaning into the decentralized approach to speed patient recruitment, increase access and diversity, improve efficiency, and capture real-world data, but are still developing protocol designs within a traditional framework. Expert DCT protocol designers, however, review trial designs to determine what aspects can be decentralized (and which cannot) and the best way to decentralize those elements. They factor DCT considerations into the process from the beginning, instead of shoehorning digital elements into the trial later or superimposing them over traditional designs.
Swing Therapeutics is a DTx company that was founded less than three years ago with $9 million in seed funding and that wrapped up $10.3 million in Series A funding in June. The company is running a hybrid trial of its investigational DTx for fibromyalgia and is expected to enroll up to 300 participants recruited from 15–25 physical sites, plus a virtual site.
The virtual site provider is remotely recruiting, screening, consenting, and enrolling participants in Swing’s PROSPER-FM trial from across the US.
By eliminating physical and geographic barriers to trial participation and execution, they have improved patient enrollment by 10x. In fact, the virtual site has surpassed all the bricks-and-mortar sites in patient enrollment.
Decentralized clinical trials are well-suited for studying digital therapeutics
Many virtual or decentralized clinical trial (DCT) specialists are successful in supporting DTx companies, as DCTs are well-suited to support prescription and non-prescription DTx studies. Fundamentally, there are no physical logistics with a DTx—no shipping, storing, chain of control, cold storage, or biohazards, and endpoints can often be captured within the DTx application itself, naturally aligning DCTs with DTx studies. Ultimately, Swing hopes for FDA-approval and will go to market.
“We are focused on getting patient recruitment right,” says Mike Rosenbluth, PhD, chief executive officer at Swing. “A virtual services model enables us to efficiently recruit participants representative of the entire patient population. It solves a huge challenge and will be critical to rapidly develop the evidence needed to bring an effective digital therapy to millions suffering from chronic illness.”
Ongoing challenges of commercializing digital therapeutics
And, while the research and development processes involved in digital therapeutics are innovative, commercializing a DTx may require more out-of-the-box thinking. Many presenters at the fall DTx East event said that even after successfully earning FDA-approval, their therapeutics are failing in the marketplace. There are new challenges to address such as lack of awareness by clinicians and their inability to easily prescribe DTx to patients.
This last challenge is uncharted territory for DTx companies. And whereas traditional drug companies average between $200–$300 million to launch a product, most DTx companies don’t have that kind of funding available to them. Plus, there are various launch challenges, patient support programs to implement, and sales and marketing teams to recruit and train.
For Swing Therapeutics and other DTx companies to be profitable or even sustainable, they need to make it easy for clinicians to prescribe digital therapeutics and get reimbursed, while also making it easy for patients to use DTx.
A new CMS code that went into effect in April 2022 will help by making it easier for commercial and Medicaid plans to cover these therapies. Yet, there are still many questions about what payment models will work best and how to get on formularies and more.
Virtual CRO Curavit raises $5m to grow digital therapeutics clinical trial business
Virtual CRO Curavit Clinical Research has tapped investors for cash, securing $5 million in series A funds to support its targeting of the digital therapeutics space.
Investors and buyers say pharma-related technologies are piquing their interest even within a tumultuous economy.
While the digital health ecosystem is anticipating a massive reset in 2023, pharmaceutical companies are willing to invest in clinical trial technology and digital therapeutics. Also, retail companies like CVS and Walgreens and payers are interested in pharma-related innovations. All this presents a potentially big opportunity for digital health investors and companies alike, experts say.
“One segment that is still eager to spend is pharma, particularly on the clinical trials sector” said Dr. Sunny Kumar, a partner at the venture capital firm GSR Ventures. According to the Digital Health Business & Technology database, companies focused on digital health trial technology have raised nearly $165 million this year across nine deals, including a $5 million investment into virtual research organization Curavit last Tuesday.
GSR’s portfolio companies include Medable, one of the industry’s biggest decentralized trial technology companies that received $304 million in funding last October. Kumar said companies like this have a tightly aligned incentive structure. “No one is truly recession proof, but companies in that space are still getting [interest] because they’re bringing a certain value proposition to the table. They’re decreasing clinical trial time and bringing drugs to market faster,” he said.”
Dr. Justin Norden, also a partner at GSR Ventures, said he prefers companies that sell to the pharma sector.
“Pharma makes decisions faster for bigger contracts with research and development focused on a return of investment,” Norden said. “If you’re a digital health company that’s going to monetize with pharma, it’s going to be a faster and easier path.”
Scott Barclay, managing director at venture capital firm Insight Partners, has invested in Trialjectory, an AI based trial matching platform that uses self-reported clinical information to facilitate clinical trial search, matching and enrollment. The company raised $20 million in a Series A round in February.
“We need to bring software and appropriate data liquidity to trials,” Barclay said. “Trials need to be better, faster, more expansive and more inclusive.”
Digital therapeutics is another area of potential investment for pharma companies, particularly as payers are increasingly willing to cover them. At the HLTH conference held last week in Las Vegas, Teva Pharmaceuticals said it was partnering with HealthTap, a virtual care management company, to expand its digital health platform. Manny Montalvo, head of digital health and innovation at Teva, said technology partnership is vital to its overall strategy on digital.
“We’re always looking to collaborate whether it’s plugging into an [electronic medical record] system, directly ordering online or something else,” Montalvo said. “If someone has better software than we do, we’re always looking to build off the platform that we have.”
Disruption in pharma is also coming from the retail side, experts say. Both CVS Health and Walgreens are investing in different technologies to create more efficient operations, including entering the de-centralized clinical trial space. Rina Shah, Walgreens’ vice president of the pharmacy of the future, said the company is also using technology to improve fulfillment, prescription renewals and medication adherence.
“Technology and analytics really drive the core infrastructure of how we deliver care all the way,” Shah said. “Our micro fulfillment center is primarily driven by technology and automation. We’re able to fulfill hundreds of thousands of prescriptions with the oversight of a pharmacist and technician onsite.”
It also has invested heavily in technology in terms of how it engages with patients. Shah said it works with both payers and providers to use “behind the scenes data” that helps the retail company better understand the patients needs.
In the area of improved pharma operations, Paul Markovich, CEO of Blue Shield of California, said the health insurance company aims to use technology to improve the pharmacy value chain. The pharma value chain is the process in which medications go to market. Companies like Blue Shield of California play an integral role as the ones who reimburse for these medications.
“We’ve laid out a vision for what a more efficient, consumer-centered pharma value chain will look like, but you’ve got to do it at scale,” Markovich said. “We’ve gone through a request for proposal but we’re still in the middle of trying to figure out which vendors could fit with our vision.”
Curavit Clinical Research Raises $5 Million led by Osage Venture Partners
This week’s Lab Notes has reports on a cancer research collaboration, a biotech startup’s multimillion-dollar seed funding round, a local firm’s investment in a virtual contract research organization and more
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Industry’s first virtual CRO that specializes in decentralized clinical trials achieves key milestones
PHILADELPHIA and NEW YORK, Nov. 14, 2022 /PRNewswire/ — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs), today announced it raised $5 million in Series A funding to accelerate its growing portfolio of research in the global digital therapeutics (DTx) market (projected to grow at a CAGR of 31.4% through 2026). The new funding will be used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription digital therapeutics trials.
The funding was led by early-stage technology investor Osage Venture Partners with additional investment from Royal Street Ventures and Narrow Gauge Ventures. It adds to early investments from Curavit founders and individual investors, including industry veterans Clark Golestani, former president of emerging businesses and global CIO of Merck, and former president and co-founder of Veeva Systems, Matt Wallach.
“In order to dramatically lower the cost and increase the speed of clinical trials, the industry must take a new, digital-first approach,” said Wallach who serves on Curavit’s board of advisors. “Curavit was founded by seasoned veterans with deep experience in that sweet spot where technology innovation meets process excellence so I’m proud to play a part in their journey to improve clinical trials.”
“This is an important milestone for Curavit and the industry’s continued momentum in digital therapeutics and decentralized approaches to clinical research,” said Joel Morse, co-founder and CEO of Curavit. “Traditional trial processes and timelines are insufficient – and they limit patient participation. New digital therapeutics are ideally suited for a DCT approach and will help improve access and drive new unique therapies to patients faster.”
The funding brings Curavit’s total capital raised to more than $8 million. Curavit has more than doubled its revenue in 2020 and 2021 and is on the same pace this year. More than half of its customer base are emerging digital therapeutics companies whose clinical research needs align with Curavit’s focus on virtual site services and DCT expertise.
“We are pleased to partner with Curavit on the next phase of their journey,” said Nate Lentz, Managing Partner at Osage Venture Partners. “The COVID-19 pandemic and rapid growth of digital therapeutics has driven a new digital model, where clinical trials are increasingly decentralized and require a new combination of technologies, services, and expertise not available in the marketplace. Curavit’s team and offering are well-positioned to fill this void and become the leading virtual CRO.”
Since its founding in late 2019, Curavit has accomplished key successes on its mission to bring clinical trials of innovative therapies to more patients in the cloud, including:
Support for important research with digital therapeutics companies, including Swing Therapeutics, Lark Health, Curio, and Sana.
Strategic partnerships with life sciences digital technology and data providers, including Ripple Science, for its direct-to-patient software platform; ixlayer, to provide easy access to clinical-grade diagnostic lab testing in DCTs; and 1nHealth, for digital patient recruitment and enrollment.
Hired experienced industry leaders in top positions including Jay Collier as COO, Candice Del Rio as director of clinical operations, and Chris O’Shaughnessy as VP of business development.
In other news, Curavit joined the Digital Therapeutics Alliance, whose aim is to broaden the understanding, adoption, and integration of clinically evaluated digital therapeutics with patients, clinicians, payors, policymakers through education, advocacy, and cross-industry collaboration.
About Osage Ventures
Osage Venture Partners (OVP) is a venture capital firm located just outside of Philadelphia, PA. It partners with exceptional entrepreneurs, building the next generation of leading B2B software and tech-enabled services companies. OVP has consistently focused on this strategy since its inception in 2005, making over sixty investments in early-stage B2B companies over that time. For more information, visit OsageVenturePartners.com.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visitwww.curavitclinicalresearch.com.
Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs), today announced it raised $5 million in Series A funding to accelerate its growing portfolio of research in the global digital therapeutics (DTx) market (projected to grow at a CAGR of 31.4% through 2026). The new funding will be used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription digital therapeutics trials.
Curavit reaps $5M in series A funding to fuel decentralized trial growth
– Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) announced it raised $5M in Series A funding to accelerate its growing portfolio of research in the global digital therapeutics (DTx) market. The round was led by Osage Venture Partners with additional investment from Royal Street Ventures and Narrow Gauge Ventures.
– The new funding will be used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription digital therapeutics trials.
In addition, Curavit joined the Digital Therapeutics Alliance, whose aim is to broaden the understanding, adoption, and integration of clinically evaluated digital therapeutics with patients, clinicians, payors, policymakers through education, advocacy, and cross-industry collaboration.
Curavit Background
Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations
Curavit reaps $5M in series A funding to fuel decentralized trial growth
The funding round was led by Osage Venture Partners with additional investments by Royal Street Ventures and Narrow Gauge Ventures, the company said in a Nov. 14 press release. To date, the company has raised more than $8 million.
The money is expected to support Curavit’s expansion of decentralized clinical trial offerings, partnerships and adoption of its CRO services and platform for prescription and non-prescription digital therapeutics trials. The company cited estimates the global digital therapeutics market will experience growth of 31.4% by the end of 2026.
“Traditional trial processes and timelines are insufficient and they limit patient participation,” Joel Morse, co-founder and chief executive of Curavit, said in the press release. “New digital therapeutics are ideally suited for a DCT approach and will help improve access and drive new unique therapies to patients faster.”
Curavit launched in late 2019, just months before the onset of the COVID-19 pandemic. Disruptions caused by the crisis initiated a global embrace of decentralized clinical trials that have become more the norm than exception.
The company also said more than half of its customer base are companies focused on emerging digital therapeutics that pair with virtual site services and decentralized clinical trial experience.
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Industry’s first virtual CRO that specializes in decentralized clinical trials achieves key milestones
PHILADELPHIA and NEW YORK, Nov. 14, 2022 /PRNewswire/ — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs), today announced it raised $5 million in Series A funding to accelerate its growing portfolio of research in the global digital therapeutics (DTx) market (projected to grow at a CAGR of 31.4% through 2026). The new funding will be used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription digital therapeutics trials.
Curavit, the industry’s first virtual CRO that specializes in decentralized clinical trials reaches key milestones.
The funding was led by early-stage technology investor Osage Venture Partners with additional investment from Royal Street Ventures and Narrow Gauge Ventures. It adds to early investments from Curavit founders and individual investors, including industry veterans Clark Golestani, former president of emerging businesses and global CIO of Merck, and former president and co-founder of Veeva Systems, Matt Wallach.
“In order to dramatically lower the cost and increase the speed of clinical trials, the industry must take a new, digital-first approach,” said Wallach who serves on Curavit’s board of advisors. “Curavit was founded by seasoned veterans with deep experience in that sweet spot where technology innovation meets process excellence so I’m proud to play a part in their journey to improve clinical trials.”
“This is an important milestone for Curavit and the industry’s continued momentum in digital therapeutics and decentralized approaches to clinical research,” said Joel Morse, co-founder and CEO of Curavit. “Traditional trial processes and timelines are insufficient – and they limit patient participation. New digital therapeutics are ideally suited for a DCT approach and will help improve access and drive new unique therapies to patients faster.”
The funding brings Curavit’s total capital raised to more than $8 million. Curavit has more than doubled its revenue in 2020 and 2021 and is on the same pace this year. More than half of its customer base are emerging digital therapeutics companies whose clinical research needs align with Curavit’s focus on virtual site services and DCT expertise.
“We are pleased to partner with Curavit on the next phase of their journey,” said Nate Lentz, Managing Partner at Osage Venture Partners. “The COVID-19 pandemic and rapid growth of digital therapeutics has driven a new digital model, where clinical trials are increasingly decentralized and require a new combination of technologies, services, and expertise not available in the marketplace. Curavit’s team and offering are well-positioned to fill this void and become the leading virtual CRO.”
Since its founding in late 2019, Curavit has accomplished key successes on its mission to bring clinical trials of innovative therapies to more patients in the cloud, including:
Support for important research with digital therapeutics companies, including Swing Therapeutics, Lark Health, Curio, and Sana.
Strategic partnerships with life sciences digital technology and data providers, including Ripple Science, for its direct-to-patient software platform; ixlayer, to provide easy access to clinical-grade diagnostic lab testing in DCTs; and 1nHealth, for digital patient recruitment and enrollment.
Hired experienced industry leaders in top positions including Jay Collier as COO, Candice Del Rio as director of clinical operations, and Chris O’Shaughnessy as VP of business development.
In other news, Curavit joined the Digital Therapeutics Alliance, whose aim is to broaden the understanding, adoption, and integration of clinically evaluated digital therapeutics with patients, clinicians, payors, policymakers through education, advocacy, and cross-industry collaboration.
About Osage Ventures
Osage Venture Partners (OVP) is a venture capital firm located just outside of Philadelphia, PA. It partners with exceptional entrepreneurs, building the next generation of leading B2B software and tech-enabled services companies. OVP has consistently focused on this strategy since its inception in 2005, making over sixty investments in early-stage B2B companies over that time. For more information, visit OsageVenturePartners.com.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visitwww.curavitclinicalresearch.com.
Curavit Clinical Research raised $5 million in Series A funding
Media Coverage | FORTUNE – Term Sheet Newsletter
November 14, 2022
Curavit Clinical Research, a Scarsdale, N.Y.-based virtual contract research organization company, raised $5 million in Series A funding. Osage Venture Partners led the round and was joined by investors including Royal Street Ventures and Narrow Gauge Ventures.
More Than One Way to Crack a Walnut: Four Fundamental Components of a Successful Decentralized Clinical Trial
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
1. Expert Protocol Design Review: What Can Be Decentralized?
Traditional clinical trials are complex, but architecting a DCT from the ground up is even more complicated. And while nearly nine in 10 sponsors say they use some elements of DCT technologies in their trials, fully virtual trials are still rare. At a recent conference, one top-10 pharma executive said that while more than half of their trial site visits are virtual, no trials are 100 percent virtual.
One reason for this is because designing a DCT protocol requires highly specialized expertise. Sponsors are leaning into the decentralized approach to speed patient recruitment, increase access and diversity, improve efficiency, and capture real-world data, but are still developing protocol designs within a traditional framework. Expert DCT protocol designers, however, review trial designs to determine what aspects can be decentralized (and which cannot) and the best way to decentralize those elements. They factor DCT considerations into the process from the beginning, instead of shoehorning digital elements into the trial later or superimposing them over traditional designs.
The best resources are experienced in clinical research, the therapeutic area of the trial, and DCT technologies. These experts know how to allocate the right DCT resources to allow for maximum patient flexibility during the trial. For instance, a lot of calendaring is often involved in planning a DCT since the patient is not tied to a specific location. It becomes critical to ensure that there are enough calendar slots for televisit appointments at optimum times for patients. A DCT protocol design expert will take all resource considerations into the design, thinking ahead about what can be done by a coordinator instead of by a clinician or registered nurse and other ways to optimize staffing.
Patient recruitment is notoriously time-consuming, but many technology-enabled firms leverage solutions specifically for a DCT. For example, one patient recruiting firm targets potential patients on digital channels using sophisticated targeting, patient-centric recruitment, and technology. Once a patient clicks on an ad, they are taken to a self-service landing page with more info about the trial and self-screening questions. If the patient passes, they can immediately schedule a live screening call, eConsent, and enroll in the trial.
One virtual CRO specializing in DCTs collaborated with this patient recruiting firm on a trial of an investigational DTx for chronic cardiovascular disease. Through targeted ads on key digital channels (i.e., Google, Reddit, Facebook, Instagram), the CRO recruited 50 patients in 10 days, surpassing the sponsor’s originally estimated four-week timeline. In addition, 39 percent of patients who clicked on an ad completed the pre-screen form – again, beating a projected 24 percent completion rate. In total, the CRI and the patient recruiting firm recruited, consented, and enrolled 150 patients in just 58 days.
“Most recruitment methods miss opportunities to enroll patients, whether in finding the right people or communicating the opportunity correctly. Expert recruitment processes coupled with technology-activated enrollment at the site and CRO levels fill trials faster with less friction,” said Dan Brenner, CEO and founder of the patient recruiting firm. “Digital recruitment allows more patients to be enrolled in the right trials, seamlessly. It breaks down the barriers between patients and studies, increasing access for more patients.”
One independent software company optimizes the use of data to digitally recruit, screen, and consent patients in DCTs. With access to 350 million lives of anonymized medical records globally, and 200 million lives of anonymized claims data in the US, the firm uses a data science-based approach to target patients across a large geography.
“In DCTs, there’s a longer-term opportunity to marry enrollment and operational data to continuously learn and refine the patient recruitment and enrollment process,” said Matt Walz, its CEO. “How else can we use this data to improve trials? For instance, this data could inform protocol development so that sponsors can better assess how inclusion/exclusion criteria might impact enrollment. All this data can improve how we work with patients.”
In the end, whichever partner supports the enrollment process, data must be aggregated on a single platform for a seamless site and patient experience, and as an opportunity for continuous improvement. “DCTs expand access to patients who live a distance from academic centers, but they can also add burden,” Rosenberg continued. “For instance, patients must decide about each visit: Does someone come to their house, do they stop at a CVS [pharmacy], or go to the clinic? It is important to consider the impact of this new experience on patients. DCT technology enables us to survey patients in real time and then find ways to alleviate any unforeseen issues.”
3. Remote Data Capture Tools: From Clinical-Grade Sensors to ePROs
The global remote patient monitoring market is projected to be worth over $1.7 billion by 2027, up 128 percent from 2021, and the increased use of a decentralized approach could push those numbers higher as DCTs require clinical-grade medical devices. Hundreds of devices already exist that capture digital biomarkers including sleep patterns, heart rate, and blood pressure. For example, continuous glucose monitors remind diabetes patients to take their insulin while allowing clinicians to monitor their disease.
In addition to these remote medical devices, DCTs can now incorporate convenient, remote lab testing with an end-to-end health testing platform. By making health testing easy for patients in a DCT, specialized firms help sponsors improve completion rates and likelihood of patient retention for the duration of the trial. One CRO partnered with such a firm for a fully decentralized trial for an investigational digital therapeutic for fibromyalgia. The firm’s health testing solution helped speed enrollment for the 12-week trial by 10 times over a traditional trial model.
“Lab testing is an integral part of most clinical trials but can compound patients’ burden in traditional settings,” explained Pouria Sanae, the firm’s CEO and co-founder. “We reduce friction for patients and sponsors by simplifying the process and streamlining data collection on the back end for DCTs.”
Electronic patient-reported outcomes (ePROs) are another critical remote data capture tool frequently used in DCTs. Look for a partner that is focused on ensuring a frictionless patient experience.
“In a DCT, patients have a larger responsibility to report their experiences even if they can do it remotely. At the same time, there is less in-person bonding where the clinician can get to know the patient’s everyday user experience. That is why it is so important to provide them with not only intuitive interfaces, but also concierge-like support throughout the trial,” Rosenberg explained.
4. Single DCT Platform: Bringing It All Together in the Cloud
So many moving parts in a DCT make it imperative to have a single platform that brings them all together for streamlined data analysis and visibility. “All DCT stakeholders need to have visibility into the entire trial journey and connect into the same system,” added Walz. “We need to provide a single entry point to trial technology regardless of recruitment source for a consistent patient experience and streamlined login for sites.”
An ecosystem of pre-vetted partners with technologies that easily integrate into a single platform can also give sponsors the confidence they need to dip their toes into the DCT pool while saving significant up-front time and money managing complex integrations. Many partnering companies and products have pre-built connectors for industry-leading DCT platforms which can drastically reduce start-up time. For instance, one CRO and its partners have reduced DCT start-up time from 14 to six weeks.
DCTs offer sponsors unparalleled trial flexibility, which is exciting in its optionality but can complicate trial design. Rather than being paralyzed by choice, start with these four fundamental elements, build from there, and remember that there is always more than one way to crack a walnut.
References available upon request.
Tips for tackling trial recruitment and retention woes in oncology
How new tools are helping companies find and keep cancer patients in clinical studies.
Oncology treatment is improving at a rapid clip, so for people with advanced cancer, a clinical trial may offer new hope when other options have fallen short. But cancer patients still aren’t signing up — a problem that has vexed the industry for years. It’s estimated that fewer than 5% of cancer patients participate in clinical trials, most of them after they have already tried another treatment first.
But trial participation can bring rewards. A study in the Journal of the National Comprehensive Cancer Network found that while only 0.01% of the 12 million patients in the National Cancer Database enrolled in a clinical trial as a first-line treatment option, those that did had better outcomes than non-participants, although they also tended to be younger and healthier than the typical cancer patient.
To help more patients take advantage of these opportunities, organizations are testing new technological tools and focusing on convenience to boost enrollment and retention, as well as diversity.
Barriers to participation
One of the primary reasons cancer patients don’t enroll in clinical trials is perhaps the most obvious — they’re unaware trials exist, said Dr. Arturo Loaiza-Bonilla, co-founder and chief medical officer of Massive Bio, a New York City-based technology company using an AI-driven platform to match oncology patients with clinical trials.
Dr. Arturo Loaiza-Bonilla, co-founder and chief medical officer, Massive Bio Permission granted by Dr. Arturo Loaiza-Bonilla
“Most patients don’t have any idea what their options are,” he said. Even when a patient is interested in participating in research, determining which trial is right for them is often a substantial hurdle. Oncologists often don’t have the time to pore through options to find the right match. It can easily take up to an hour to go through all the criteria and data to search for a trial for one patient, Loaiza-Bonilla said. Some larger practices may have research coordinators to navigate this process, “but in a community practice, you don’t have that luxury, (and) you don’t have that person or expertise,” he said.
Oncology trials typically require patients to meet very restrictive participation parameters, ranging from the genetics of their cancer to the type of treatments they’ve previously undergone.
“Getting into a clinical trial for oncology is extremely challenging because there are so many criteria required,” Loaiza-Bonilla said.
Finding the right match takes an intensive approach, and as a result, many patients miss out.
“It has to be almost like a real-time activation for the patient. And if there’s no system to do it in real time for you, no one’s going to help you,” he said.
There are also emotional challenges and logistical barriers to contend with, said Candice Del Rio, director of clinical operations for Curavit, a virtual CRO that operates decentralized clinical trials. When a patient receives a cancer diagnosis, they are already overwhelmed, which may make them reluctant to take on additional treatments. She saw this firsthand as a nurse working with participants in oncology clinical trials. For patients still processing that initial shock, the idea of participating in research may seem like an additional burden.
“They may say, ‘Look, I just got to the hospital. I’m overwhelmed. I just need some downtime. I don’t know that I want to do anything extra. I just kind of want to stay the course,’” Del Rio said.
Organizations need to take steps to address these barriers if they want to increase enrollment.
Strategies to boost enrollment
Massive Bio is tackling the problem by enlisting tools to help patients more easily find the right trial.
“We founded the company with the goal of making clinical trials accessible for all cancer patients no matter where they are, and using technology at scale to make it work,” said Loaiza-Bonilla. “The space is already crowded by a lot of people saying we’re going to try to solve the problem, but there’s no good engine that’s able to connect the dots, and that’s what we’re aiming for with the company.”
Massive Bio’s AI-driven technology, the Deep Learning Clinical Trial Matching System (DLCTMS), pairs patients with existing trials in the ClinicalTrials.gov national database by combing through medical records to find the most clinically appropriate options based on the specifics of their cancer, including biomarker data. The company’s platform, which has onboarded 100,000 cancer patients to date, also includes other factors in its algorithm, such as the trial location, the patient’s insurance coverage and social determinants of health, Loaiza-Bonilla said. It ranks up to 100 exact and partial matches.
“We’re able to in 17 seconds match you to all the trials available in real time,” he said. Getting this information quickly is crucial because all too often a patient might find out too late that they were a match for a particular trial that has ended enrollment.
The system can also flag potential trials the patient might qualify for down the road if their condition changes, Loaiza-Bonilla said. “We are basically putting together a list of options that you can activate in real time,” he said. “The nice thing about it is that if you are on our platform from the beginning, we can help you across your journey.”
The goal is to help more people — and importantly a more diverse group of people — participate. Increasing broad participation in research has become even more crucial in light of FDA guidance aimed at increasing diversity in clinical trials, Loaiza-Bonilla said.
Retention is crucial
However, simply getting patients into trials isn’t enough — organizations need to retain them, Del Rio said. This is where decentralized trials can excel.
Candice Del Rio, director of clinical operations, Curavit Permission granted by Candice Del Rio
Patients with cancer are already dealing with a lot and need trial options that more easily fit into their lifestyle. For instance, many patients Del Rio has worked with needed to travel from other states or even other countries to participate in a study, making the process difficult and expensive and, in some cases, requiring patients to find temporary housing. Decentralized trials can make the process easier on patients by allowing them to participate from home, requiring fewer site visits.
One reason people running clinical trials hesitate to embrace a remote option because they have less in-person contact with patients, Del Rio said. But remote trials can also offer advantages when it comes to tracking patient health in real time.
“You can get quicker notifications. Sometimes in a clinic, we wouldn’t know that someone was experiencing an adverse event for two weeks until they actually came into the clinic,” Del Rio said.
But remote monitoring allows researchers to quickly identify when something is off and respond quickly. This can also improve retention, she said, because a patient with a new symptom can get immediate help, which might otherwise lead them to abandon the trial.
When using a decentralized model, however, it’s important to incorporate some flexibility in your trial design, Del Rio said. For example, while technology can be more convenient for some trial participants, it may sometime be challenging for others. Providing options can help.
Building for the future
Overall, improving enrollment and retention in oncology trials is crucial.
“Trials are part of the treatment. In a lot of ways, it’s the gold standard because drug developers are constantly trying to find better ways to treat an illness and cause fewer side effects and prolong longevity,” Del Rio said.
While there are many reasons why patients don’t participate in trials, improving enrollment often comes down to two simple factors — improving access and communication.
“If we use [our] tool at scale and reach out to those populations, we can hopefully make studies much more accessible to those populations that otherwise may have not been able to get them,” Loaiza-Bonilla said.
Curavit partners with 1nHealth for digital first recruiting of DCT
Digital enrollment for Lark Health’s Cardiovascular Disease DCT is sped up by using the “tapestry of the entire internet” through Curavit and 1nHealth.
Bringing your whole and authentic self to work is key. But what does that mean? And why is it important to have a personal leadership brand?
Experts say a brand conveys your identity and distinctiveness as a leader, communicates the value you offer, positions you as an industry thought leader and enhances your company’s brand. It can also give people a reason to follow you. As John Maxwell said: “If you think you’re leading, but no one is following, then you are only taking a walk.”
Your leadership persona should tap into your key attributes, talents and skills, but it might seem daunting to figure out what that brand should be. In a Forbes article, Devapriya Khanna, founder and CEO of 212° Brand Lab, laid out three brand builders: expression, emotional intelligence and executive presence.
First, “identify your values, vision, purpose and goals and package them into an authentic expression — so that your signature style and voice are unique, yet consistent.” Second, use self-awareness as the basis for emotional intelligence. Finally, she noted a “mindful and focused leader exudes leadership presence. Mindfulness can open the door to emotional connection with oneself and others.”
Take the time and put in the effort to create the persona that reflects your reputation as a credible and trustworthy leader who others will follow to achieve the big, hairy audacious goals for your organization.
For insights on how life science executives view their leadership style, we asked our 2022 PharmaVoice 100 honorees to identify the brands they relate most with. It’s no surprise that many pointed to top global brands — Apple, Google and Amazon — as inspiration. Interestingly, Patagonia was the No. 1 brand identified, with execs noting the company’s commitment to social responsibility, sustainability and community as values that resonate with them.
Here’s what some of the industry’s top execs had to say about their personal leadership brands.
Apple to the core
“I see Apple as a brand that is fueled by creativity, innovation and disruption. It’s a company that has pushed boundaries and been forward thinking since its beginning. I aspire to drive disruptive and innovative ideas forward, and foster the curious, creative mindset that seems to be the core of the Apple brand.”
“Apple, because they are always striving to add value for their customers while being unrelenting in their pursuit of it.”
Jennifer Gould, director of marketing excellence, GSK
Permission granted by Jennifer Gould
“If I were to brand myself, I would integrate the positive aspects of Google into my brand. For example, Google is widely accessible to so many people all over the world and as a champion of the decentralized model for clinical trials, one of the key benefits of that model is to make clinical trials widely accessible to all demographics. As DCTs continue to gain momentum, they will enable greater diversity and inclusion for trial participants.”
Dr. Pamela Diamond, co-founder and chief medical officer, Curavit Clinical Research
Permission granted by Pam Diamond
“Google, because it is colorful and doesn’t take itself too seriously but represents clear technical excellence with world changing impact
Armon Sharei, founder and CEO, SQZ Biotechnologies
Permission granted by Armon Sharei,
“I would choose Ben & Jerry’s ice cream. There are several reasons why this is the perfect choice for me. Ben & Jerry’s has a long history of supporting and promoting social justice issues. I have tried to do the same. Ben & Jerry’s co-founders have made it their mission to protect the environment and promote sustainable food systems. Moreover, Ben & Jerry’s has supported free trade and partners with equity-related organizations. The causes Ben & Jerry’s focuses on deeply resonate with me in my life and my career. Promoting social justice in everything we do, ending systemic racism in healthcare, being a vegetarian and protecting the environment are vital to me. Finally, I love ice cream.”
Lori Abrams, former vice president, patient advocacy and clinical research diversity, WCG
Permission granted by Lori Abrams
“My brand would be Disney because they put customer service above all else to ensure everyone has an amazing experience. They don’t always get everything right, but they always listen to their employees, shareholders and customers and seek out their feedback for improvements.”
“If I were a brand, it would be The North Face. Outside of the great products they offer, the company’s mantra ‘Never Stop Exploring’ has always resonated with me. Named for the most challenging side of the mountain, the company has always encouraged its customers to push their limits, discover something new, and reach their dreams. While Karuna operates in a completely different market, we also encourage exploration, innovation and pushing the boundaries of what is possible to bring meaningful new treatments to people who need them.”
Andrew Miller, founder and chief operating officer, Karuna Therapeutics
Permission granted by Andrew Miller
“Patagonia: Their values are at the forefront of everything they do; their actions reflect their mission and values. With a focus on sustainability, quality, education and activism, they want to build the best products, cause no unnecessary harm, in the process and use their business to inspire and implement solutions to the environmental crisis.”
Dr. Barbara Klencke, chief medical officer, Sierra Oncology, a GSK company
Let’s face up to facts – there are challenges when it comes to clinical trials. Patient recruitment can be challenging and dropout rates can be high. Studies often put significant pressure on patients, who must juggle personal commitments with travel and trial participation.
Working with virtual CROs, explains Joel Morse, CEO at Curavit, could be one solution to the multitude of challenges companies face. “The traditional model for clinical trials has worked well for a very long time – and it still does serve a purpose,” says Joel Morse, CEO at Curavit – a virtual CRO. “However, it is inherently complex, with multiple sites, multiple and disparate patient recruitment efforts, and multiple places where data resides. The biggest challenge remains finding patients.”
Morse is passionate about the benefits of using digital tech to improve trials. For example, digital technologies can allow patients to participate in a trial regardless of location. For example, televisits allow patients to meet with the principal investigator of the trial from anywhere via a simple web link. “Patients can report how they’re doing to trial teams via electronic diaries rather than having to go into a doctor’s office,” he says. “They can also handle the often long process of consenting to participate in a trial through e-consent applications and report on progress via e-PRO technology or electronic patient-reported outcome solutions.”
Morse also adds that technologies can enable companies to solve big challenges that are important to regulators and government, including diversity, health equity, and patient centricity. Digital technologies expand patient access to clinical trials across a wide geography because patients are no longer tied to physical trial site locations. Most trials take place at large academic institutions or academic hospitals in major cities, making it logistically difficult, if not impossible, for patients in rural or remote locations or without the financial means to take off work and travel great distances to participate. In fact, 70 percent of all clinical trials worldwide occur at just 5 percent of research sites, which primarily draw patients from populations within 40 miles of trial sites. Digital or DCT technology allows patients to participate from their own homes, eliminating the barrier of travel.
He says, “In my view, the most exciting potential of virtual trials is the ability to reach the large percentage of patients that are not historically exposed to clinical research. Virtual trials are also one of the rare instances where the regulatory environment is providing tailwinds to innovation by creating new guidelines for digital tech use in trials so they can certainly add value to trial recruitment and retention.”
But this does not mean that virtual trials are a panacea to all of the industry’s clinical trial issues. “Sometimes sponsors will try to incorporate digital technologies into a traditional trial that was not initially designed for digital. This has the unintended consequence of pushing new technology onto the trial sites without properly training them how to use it from the beginning, complicating and even slowing down the trial mid-swing,” Mose says. “If companies designed trial protocols by collaborating with DCT experts from the beginning by looking at what aspects of the trial could benefit from decentralization and building those technologies and processes in early, you have the best results.”
But Morse is optimistic about virtual trials. But believes further progress will be necessary to see their widespread use. He says, “Currently too many trials shoehorn technology into a traditional design and end up increasing, not decreasing, patient burden. One day, digital technologies and processes will be an integral part of all trials, natively designed into each one.”
Digital enrollment for Lark Health’s Cardiovascular Disease DCT is sped up by using the “tapestry of the entire internet” through Curavit and 1nHealth.
The pharma industry is full of execs who were initially inspired to pursue a career in healthcare after seeing a doctor in action. But not many can say this interest stemmed from up-close encounters with a doctor from the von Trapp family — the family who formed a singing group together and were the inspiration behind “The Sound of Music.”
When Dr. Pam Diamond was growing up in a tiny Rhode Island town, her parents fought chronic health conditions for years while being cared for by Dr. Rupert Georg von Trapp — the oldest of the original seven Austrian von Trapp children who formed the Trapp Family Singers with their parents, Georg and Agatha.
“I was inspired to make medicine my career from witnessing Dr. von Trapp make such a difference in the lives of both my parents,” Diamond says. “He was a superb clinician.”
Diamond had her first encounter with disparities in expectations when she told her high school guidance counselor that she wanted to go to medical school, but was encouraged to pursue nursing instead. Of course, Diamond didn’t listen and not only succeeded in medical school, she soared, breaking down barriers as the only woman in her general surgery internship and then as the only woman resident during the last two years of her otolaryngology training.
After practicing medicine for almost 30 years, Diamond “decided she wanted to make a broader impact on healthcare by modernizing clinical trials,” her nominator says.
Seeing opportunities to innovate in the field, Diamond co-launched Curavit Clinical Research in 2019. The timing could not have been more challenging — and more apt. Although the pandemic brought clinical trials to a halt around the world, Curavit emerged with digital solutions just in time, becoming the first all-virtual contract research organization (VCRO). According to her nominator, there were only 617 decentralized clinical trials (DCTs) with a virtual component in 2019. In the space of just three years, that number has now swelled to 1,300 trials.
“And the benefits on clinical trial speed, access and patient diversity — even outcomes — are becoming clear,” her nominator says. “Maybe as important, the adoption of DCTs has opened a new level of innovative thinking in how clinical research gets done.”
“Undoubtedly, COVID-19 helped DCTs gain acceptance among sponsors, investigators and participants. But now stakeholders are seeing the incredible advantages of this new digital model to drive acceptance post-pandemic and beyond.”
Dr. Pam DiamondChief medical officer, co-founder, Curavit Clinical Research
To stay successful in the quickly evolving space, Diamond says she has relied on decisive thinking.
“DCTs rely heavily on technology,” she says. “If trial design decisions are not made expeditiously, the originally proposed technology solutions could become obsolete.”
DCTs have not only brought more speed and efficiency into the trial space, they’ve also been a boon for patient diversity. Diamond’s nominator notes that Black patients comprise just 5% of the research population, even though they account for 13.4% of the total population in the U.S. Yet, Diamond believes virtual DCTs may help level the research field — just one of several key advantages DCTs bring.
“DCTs provide greater access to trials, reduce trial budgets, improve population representation in trials and make rare disease research dramatically more feasible,” Diamond says.
To date, Diamond’s nominator says one of the company’s most successful efforts has been in remote digital technologies to test a hearing loss treatment developed by a Boston area biotech company.
“[Diamond] and Curavit’s Lead Audiologist, Dr. Rachel Rangel, designed a unique way to record the audiometric evaluations of patients across all sites with the recordings automatically uploaded to a cloud-based platform, accessible to the Curavit team for objective endpoint adjudication,” her nominator writes.
As an “unassuming, behind-the-scenes innovator,” Diamond’s nominator says these new approaches are being pushed forward because Diamond “replaced her white coat for a suit coat” to connect more patients to clinical trials.
Curavit, Swing team up on fibromyalgia therapeutic trial
The CRO and DTx specialist are joining forces to conduct a hybrid clinical trial of a potential digital therapeutic that is aimed at treating fibromyalgia.
For Digital Therapeutics, Virtual Trials Leverage Efficiencies
The virtual format is catching on but has important limitations which make it unsuitable in certain situations.
The promise of prescription digital therapeutics (DTx) is the opportunity to use the ubiquitous technology to quickly and efficiently deliver therapies to patients. Increasingly, the makers of digital therapeutics are seeking to leverage those same efficiencies to streamline clinical trials.
Earlier this summer, Swing Therapeutics announced it had hired Curavit Clinical Research to be a virtual site for the pivotal trial of Swing’s investigational fibromyalgia digital therapeutics.
Under the terms of the arrangement, Curavit will recruit, screen and enroll patients into the PROSPER-FM trial, after which Curavit will manage participants over the course of the trial’s 12 weeks. The trial involves the study of 2 digital applications, which incorporate combinations of self-management skills, mindfulness activities, symptom tracking, and disease education.
oel Morse, MBA, Curavit’s chief executive and co-founder, told Managed Healthcare Executive® that digital therapeutics are a natural fit for virtual trials.
“There are no physical logistics — no shipping, storing, chain of control, cold storage, or biohazards, plus endpoints can be captured within the digital therapeutic application itself, making DCTs [digital clinical trials] ideal for studies whether seeking regulatory approval or consumer and payer confidence,” he said.
Morse said another benefit to digital trials for digital therapies is that the products by design track the most of the relevant endpoints of the trial. As a result, he said, digital therapeutics makers can avoid the need to purchase expensive third-party software to track endpoints.
That said, the virtual format is not a fit for every scenario or indication. Without a physician or other healthcare provider directly monitoring patients in clinics, certain endpoints cannot be feasibly or reliably measured in a remote setting.
Mike Rosenbluth, Ph.D., the CEO of Swing, said the fibromyalgia trial will avoid such problems because the endpoints being studied are based upon patients’ daily experiences of the disease.
“Understanding patient outcomes in their day-to-day rather than in a provider clinic is more accurate and representative of how well they are doing,” he said.
Rosenbluth said the endpoints in PROSPER-FM are all patient-reported, which is the accepted “gold standard” for fibromyalgia studies, he said.
“Even if we conducted all in-person visits, we would still collect these outcomes remotely,” said Rosenbluth.
But Rosenbluth said one benefit of the virtual design is that patients do not have to travel to receive their therapy, which is important because the condition itself can make travel uncomfortable and difficult.
“These patients can be in pain and fatigued and it is unreasonable to ask them to take on another task when getting through their day is already hard,” he said.
One of the most important facets of any critical trial is recruitment. Studies with an insufficient number of enrollees or with enrollees who do not reflect the demographics of the real-world patient population may have limited generalizability and ultimately, limited usefulness. Rosenbluth said a virtual structure can also help in this regard.
“This approach absolutely makes it easier to get a representative sample for our study population,” he said. “This has been a real challenge in previous studies in the field.”
As for the broader potential of virtual trials, Morse said it is important that any potential virtual trial be evaluated carefully for its suitability, including “taking a cautious look at things like high morbidity patient populations, complex therapies, and significant physical and/or emotional safety concerns,”
In some cases, traditional or hybrid approaches will still be most appropriate, he said.
Video: The State of Decentralized Clinical Trials | Interview
What can pharma companies do to ensure that clinical trials are conducted in the most efficient and patient-centric manner?
Clinical trials are integral to the drug development process. Yet, they are still affected by long-standing challenges, including poor recruitment and retention, the use of paper-based systems, and siloes among participating stakeholders. Though many in the industry agree that something must be done to address these challenges, practical steps are necessary to see real and lasting change.
The Medicine Maker brought together an expert panel to discuss the challenges affecting clinical and what can be done to make a difference.
Watch our video to learn more about the trends and challenges affecting clinical trials, including the growing prevalence of digital and decentralized trials, COVID-19 induced supply chain issues, and the impact the war on Ukraine is having on trials.
Participants:
Georg Schulz, EVP of Clinical Services & Senior Director of Corporate Development at Tanner Pharma Group, a global provider of pharmaceutical solutions.
Georg has more than 25 years of senior executive experience in the pharmaceutical industry. He has a proven track record in strategy design and execution, organizational development, supply chain management, international air and sea transport, and cold chain management for pharmaceutical products.
Dave Hanaman, President, Co-founder, and Chief Commercial Officer at Curavit
Dave co-launched Curavit over two years ago. He has spent more than a decade as an intelligence officer in the US Navy and was co-founder and director for 22 years of C3i, a global healthcare technology company, until it was sold.
Claire Marsden, VP, Digital and Decentralised Solutions at Medable
Claire has worked in the industry for over 25 years. She has worked across all phases of clinical development in companies including GSK, Pfizer, Novartis, Bayer Alnylam, and IQVIA.
Andrea Valente, Chef Executive Officer at ClinOne
With over 20 years of industry experience, Andrea joined ClinOne after serving as Chief Operating Officer at Medable. She has an extensive background in life sciences technology product development, delivery operations, customer loyalty, and merger and acquisition strategy.
Unique Considerations in Designing Decentralized Trials for Digital Therapeutics
Digital therapeutics (DTx), the use of software-based interventions to prevent and treat disease, is one of the biggest areas of growth in life sciences. CB Insights reported that 2021 funding in the digital health industry grew 79% over 2020,{1} and the global DTx market is projected to hit $13.1 billion by 2026, up from $3.4 billion in 2021.{2} Many say digital therapeutics will re-write the future of healthcare.{3}
The DTx industry isn’t just aspirational. Studies show improved outcomes from DTx, either alone or in conjunction with conventional therapeutics, in a broad range of indications, including cancer, ADHD, asthma, schizophrenia, and insomnia. Some examples of products include video games to treat mental and behavioral health issues; a platform that incorporates neurological music therapy, sensors, and artificial intelligence to help patients who have suffered a stroke or other neurological disorder to rebuild motor skills; and a smartphone app that can conduct electrocardiograms anytime, anywhere.
Background
While exciting, this is still unchartered territory. Regulatory lines are often blurry between prescription DTx, non-prescription DTx, and combination digital therapeutics/traditional medication. It’s worth noting, however, that the U.S. Food and Drug Administration (FDA) has demonstrated its commitment to supporting digital health technologies through the publication of multiple guidance documents and the launch of the Digital Health Center of Excellence, which aims to connect and build partnerships to accelerate digital health advancements, in September 2020. In April 2021, too, the FDA loosened regulations surrounding approval of digital mental health tools to hasten their time to market.{4}
Even so, not all DTx manufacturers choose to seek FDA approval, but they all need to prove efficacy through clinical studies for payers to consider coverage and consumers to consider purchase. Regulatory approval is not always the end goal—or at least, not initially.
AstraZeneca, for instance, has designed a rigorous and low-patient-burden digital therapeutic to monitor metastatic breast cancer patients. The prescription DTx, which is currently being tested in clinical trials in 23 countries, was developed using insight from a review of medical literature, pulmonary and breast cancer experts, technology review, and real-world evidence gathered through conducting a deep cohort analysis of approximately 500 patients in U.S. health systems.{5} The therapeutic’s aim is to monitor patients’ symptoms and vital signs and, based on algorithms and expert rules, alert a physician as to how well the patient is doing on the treatment to maximize both safety and outcomes.
“Regulation will differentiate between a fitness app a consumer can simply download, with no regulation required, versus something that is scientifically proven to have a direct impact on someone’s health condition or outcome, which a doctor may prescribe,” said Cristina Duran, chief digital health officer for AstraZeneca, in a statement. “In a few years, I think we will see that shift to it being commonplace for your doctor to prescribe a digital therapeutic, a medication, or both.”
Indeed, it’s a complicated and quickly evolving arena in healthcare.
On top of the current regulatory limbo, DTx manufacturers face many of the same clinical trial challenges as traditional drug makers, including those tied to patient recruitment and retention, quality of data, and costs. They also must carefully consider the unique technical security concerns of an all-digital therapeutic and face strategic decisions around either provisioning smart devices or leveraging a “bring your own device” (BYOD) policy. At the same time, clinical trial models are rapidly evolving, adding further complexity for companies working to develop innovative digital therapeutics in a post-pandemic environment. Decentralized clinical trials (DCTs) are becoming a preferred model for research in biopharma and offer even greater benefits to companies conducting studies on digital therapeutics.
Wave Neuroscience, a medical device manufacturing company that specializes in designing software and physics-based personalized brain-based interventions, is moving toward more decentralized clinical trial designs. “DCTs can improve patient recruitment and retention by reducing burden and eliminating geographic barriers,” explained Dr. Erik Won, president and chief medical officer of Wave. “This also results in a more representative sampling of the population, such as patients from rural areas who often don’t have access to major institutions.”
Dr. Won continued, “DCTs can also increase the quality of data by minimizing the Hawthorne Effect—where individuals modify an aspect of their behavior in response to their awareness of being observed, also known as ‘white coat syndrome’—because patients are in their home environment.” Finally, DCTs can be more cost-effective, he added.
When Stars Align: DCTs and DTx
Fundamentally, a DTx is software rather than a pill or injectable, so there is no distribution or administration of medicines. There are no physical logistics—no shipping, storing, chain of control, cold storage, or biohazards—plus endpoints can be captured within the DTx application itself, making DCTs ideally suited for DTx studies whether the goal is regulatory approval or consumer and payer confidence.
In all cases, though, the unique advantage is that the DTx being studied in a trial is also the data collection device, so manufacturers often don’t need extra technologies like an electronic patient-reported outcome (ePRO) system to capture data in a clinical trial. It’s all in one, and this can result in big cost savings.
For example, Texas A&M and Wave Neurosciences are conducting a hybrid clinical trial on the safety and efficacy of magnetic EEG-guided resonance therapy to treat post-traumatic stress disorder (PTSD). This therapy uses transcranial magnetic stimulation, which has been cleared by the FDA for treatment-resistant major depressive disorder, obsessive compulsive disorder, and nicotine cessation. With this algorithm-driven therapeutic, a personalized treatment is delivered via conventional (in-person) appointments. Screening and follow-up visits, in which participant-reported data are collected, take place virtually to the extent possible.
“America is experiencing a crisis in mental health,” said Dr. Won. “Software- and physics-based personalized therapeutics are a modern, non-pharmaceutical, non-invasive option to help in this area. We are testing our therapeutic with an eye to pursuing an FDA marketing approval for the PTSD indication. We are exploring the decentralized trial model to introduce greater flexibility and speed into our research efforts.”
Best Practices for Designing DTx Trials
With the quickly growing and evolving DTx market, and the complexities associated with clinical research, here are five considerations for decentralized trial design:
Know your regulatory roadmap before embarking on a trial.
Because the regulatory pathway for digital therapeutics is not as clear-cut as it is for traditional investigational drugs, it is critical to outline your regulatory roadmap before recruiting the first patient. Feasibility studies can be a good place to start, especially to help map out an expansion plan down the line. Some important considerations also include how future versions of your DTx product will be tested, benchmarked, and evolve over time.
“It is always best to seek meetings with the FDA’s device division [the Center for Devices and Radiological Health] early, and often,” said Dr. Daniel Karlin, chief medical officer at MindMed, a clinical stage biopharmaceutical company developing novel products to treat brain health disorders. Dr. Karlin is also the lead medical advisor to the makers of the first and only FDA-cleared, prescription DTx that improves sleep in adults 22 and older with nightmare disorder or nightmares related to PTSD.
Dr. Karlin continued, “It is easier for DTx providers to secure meetings with the FDA because digital therapeutics are typically less biologically complex and therefore pose less risk. Request a meeting at the start of your development efforts to agree on the claims you plan to make based on the indication for use, and to establish what related evidence will satisfy the FDA. This is fundamental. Also, seek institutional review board [IRB] clearance on anything that could conceivably be research-related before you bring an experimental device to humans for studies.”
Of course, regulatory approval—while often considered the ultimate validation for the safety and efficacy of a drug or device—isn’t the only reason for conducting clinical research, especially with DTx. Health economic outcomes and human factor research are often equally important for product adoption. Even in the digital realm, real-world function and outcomes are important to create products that lead to meaningful outcomes for patients. “All manufacturers want payers and patients to be confident in our product’s efficacy, safety, and economics,” added Dr. Won.
For instance, some DTx products that have minimal risk may not require regulatory approval but are just as valuable as those that do. Decide if regulatory approval is on your short-term or long-term roadmap and design the trial accordingly. If it is not, then there is greater flexibility in study design.
Map out an immediate and long-term commercial strategy.
Given how quickly the DTx marketplace is evolving, the best that can be done may be to sketch out a preliminary commercialization strategy that has plenty of leeway to deviate from that path, if necessary. For instance, if your therapeutic will not be intended for regulatory approval, you may need to focus on a consumer strategy that focuses on everyday wellness. If you know this up front, you can design your clinical trial around endpoints that mirror your target consumer’s biggest pain points. However, if your end-goal is to develop a DTx that will be used in combination with an FDA-approved drug, then you will need to design your trial based on endpoints relevant to that drug maker’s target patient population.
Carefully consider and incorporate protections against technical security breaches.
Data security and privacy are crucial for all clinical trials, but especially when studying DTx that are 100% tech-driven and, therefore, potentially vulnerable to more issues. One of the most important decisions that needs to be made up front is whether the protocol will strictly enforce a BYOD strategy (which could prevent some patients from participating) or require the sponsor to provision devices to all participants (which could be cost-prohibitive)—or some combination thereof. Each option comes with different security considerations, so decide this up front.
Regardless of device strategy, all data collected on the smartphone will need to be encrypted and then sent to a secure central platform in the cloud that follows all regulatory compliance parameters. Additionally, invest in a platform provider or tech-enabled CRO that maintains a strict security perimeter, including a “zero-trust” architecture with individual logins and audit trails for everyone who has access to the data every time they log in or out—this, on top of the digital therapeutic app’s security standards.
Develop digital endpoints that are fully validated and meaningful to patients.
Traditional medicine trials measure against accepted endpoints that are validated in accordance with standards set forth by the IRB and regulatory organizations. However, DTx studies are typically measuring novel digital endpoints that are different for each DTx app and do not have a history of vetted benchmarks against which to be validated. Even so, reviewers will need to ensure that the novel endpoints aren’t bogus, and this can require some extra steps and creativity.
In many cases, endpoint validation in DTx studies requires a comparison to something similar that has been already validated or the use of previously vetted ratings scales. For example, when conducting a depression study, the DTx sponsor may first administer the Columbia-Suicide Severity Rating Scale—a suicidal ideation and behavior rating scale created by researchers at Columbia University, University of Pennsylvania, University of Pittsburgh, and New York University—to potential participants at screening. The patient’s score can be the baseline for the study, so if the DTx is efficacious, that score should drop and serve as a validated digital endpoint for symptoms of depression.
Similarly, DTx studies may leverage ePROs to administer quality-of-life questionnaires compared against prior research already accepted and validated by the IRB and FDA. Another way to validate endpoints in a decentralized DTx trial is to incorporate an initial site visit with a clinician who can compare the measurement of, say, a wearable device against an equivalent onsite, hospital-grade machine. Doing so can prove the wearable is as valid a measuring tool as another.
Finally, as important as endpoint validation is patient validation—in other words, identify the measurements or endpoints that are meaningful to patients. For example, with Fern Health’s digital musculoskeletal platform, the company shifted the focus of pain management from pain relief to functional restoration. Early on, the company found that functional pain endpoints are more important to patients in the long term than pain relief alone and made that critical adjustment.
Assess the use of DTx placebos or sham apps early and often.
In a DTx clinical trial, dummy or “sham” apps are often used as a control in comparison to the actual treatment or intervention app—like a placebo pill used in a randomized control trial. There are unique considerations in using sham apps, however, including the potential for an unintentional placebo effect.
Here is the challenge: It is very difficult to make a sham app similar enough to the real one, which means patients often suspect that they were not assigned to the treatment arm. In addition, patients who do interact with the sham app can experience a placebo effect that negatively skews study results. For instance, patients in the treatment arm of a study would typically show significant symptom improvement compared to the non-treatment arm, but when using a sham app, that disparity is not as dramatic.
The FDA has not yet ruled on whether placebos or “sham” apps must be used in DTx trials, but the agency often prefers a sham control. DTx companies that opt not to use a sham control will need to work very hard to find creative ways to design an FDA-acceptable trial that won’t be criticized—even then, there is no guarantee that the FDA will accept the results.
“It is highly unusual to view sham controls as unnecessary in clinical trials,” said Dr. Karlin. “Not only do regulatory bodies prefer sham-controlled evidence in digital therapeutics studies, but also clinicians. Reluctance to use sham apps will cause companies to struggle to get both FDA clearance and physician buy-in, which is critical for commercial success with patients.”
Dr. Karlin’s team for the PTSD DTx leveraged a sham control on a wearable device that, rather than buzz when detecting a nightmare, simply recorded it. “When we assessed the reliability of our blind through a survey of our trial participants, we found that most did not know whether they were using the real therapeutic or the sham,” he noted. “This helped validate the research because it meant that we could reliably compare the active intervention with the placebo for more meaningful results. Randomization and sham control are not magic bullets, but they’re the best options we have right now.”
As the Digital World Turns…
There’s still a lot to be learned in the DTx market, but they are here to stay with growing reliance, trust, and adoption of digital health products. COVID-19 pushed researchers to lean into the decentralized model for research, and the pandemic has simultaneously fueled a growing need for DTx products—an ideal marriage of process and product. Remaining flexible and open-minded will be critical to succeed in this evolving and exciting area—as the digital world turns.
References
Taylor NP. 2022. Digital Health Funding Jumps to New High. MedTech Dive. See full resource here.
Market and Markets report. 2021. Global Digital Therapeutics Market Projected to Reach USD $13.1 Billion by 2026. ReportLinker. See full resource here.
Taranto B. 2021. The Growing Power of Digital Healthcare. TechCrunch. See full resource here.
Staff report. 2021. DTx Trends and Companies to Watch in the Growing Digital Health Industry. Insider Intelligence. See full resource here.
Galbraith S. 2021. Digital Therapeutics: Augmenting Patient Outcomes. AstraZeneca. See full resource here.
Digital Therapeutics Deliver Surprising New Benefits for Cancer Patients
Digital technologies have had profound effects on how we communicate (i.e., smartphones), share information (i.e., social media), and create (i.e., 2- and 3-D printing). Now, they are having an impact in healthcare, too. The latest (and arguably most exciting) example is digital therapeutics (DTx): medical treatments to address health conditions via a combination of software and communications. DTx are in use or being tested for a growing list of diseases and conditions: Type 2 diabetes, congestive heart failure, obesity, Alzheimer’s disease, dementia, asthma, substance abuse, hypertension, anxiety, depression, and more.
Digital Health or Digital Therapeutics?
Researchers and policymakers make distinctions among digital health (the overall category of health-related interactions), prescription digital therapeutics (apps or tools that have gained regulatory approval), and software used as an adjunct to guide a healthcare provider’s treatment of a patient (software as a medical device, or SaMD, regulated in the US by the FDA Center for Devices and Radiological Health). There are overlaps from one category to another but, in nearly all cases, a rigorous evaluation in the form of a clinical trial to clearly demonstrate the impact of the digital technology is needed, even when regulatory approval is not the end goal.
“Digital solutions have a variety of intended use cases which drive their approval pathway, and they are equally valuable and important depending on the end goal,” said the head of digital health, oncology R&D at a top-10 pharmaceutical company that has digital therapeutics in development across therapeutic areas. “Whether the digital therapeutic is for consumer health assessment or in a trial or routine care setting, following the guidance around use cases and a carefully developed measurement framework is critical to ensure scientifically rigorous and responsible assessment of a patient’s health status.”
In parallel with the maturation of DTx, numerous researchers have been examining the social or patient-centered aspects of oncology care, especially now that oncology care is becoming a participant in the DTx evolution. The opportunities for improving health outcomes in oncology through DTx arise from challenges expressed by many cancer patients: surgery, radiation, chemotherapy, and/or immuno-oncology, all carried out over several years and with substantial side effects. Sleep, eating patterns, and physical activity can be affected. For many patients, simply withstanding the course of treatment is a victory, let alone what happens to their cancer.
Researchers think that digital therapeutics can help. One pre-market prescription DTx company dedicated to improving mental health in cancer patients is conducting various clinical trials on new DTx products designed to improve cancer-related distress that affects a patient’s quality of life or ability to cope with cancer diagnosis and treatment, which affects nearly half of cancer patients. According to the company, “digital therapeutics that help to treat cancer-related distress have the potential to help close the cancer treatment gap.” DTx products may incorporate cognitive behavioral stress management, which has been tailored to cancer patients and shown in numerous clinical studies to improve emotional well-being, physical health, and overall survival.
“We will continue to prioritize the study and development of digital therapeutics for real-time, continuous patient monitoring, from side effects of treatment to symptoms of disease that indicate progression. The aim is to allow patients to stay on therapy longer, have fewer side effects and adverse events, wherein this improved treatment tolerability may potentially lead to increased benefit from therapy,” added one top-10 pharmaceutical company’s head of digital health.
For at least the past decade, researchers have been documenting longer survivals, better adherence to therapy, and improved quality of life (QoL) when various forms of digitized health or therapeutic actions are taken. A lung cancer study comparing symptom monitoring using a DTx versus the standard process conducted in France in 2017 was so successful that it was prematurely halted and patients in the control group were transferred to the study group receiving the digital intervention. The median overall survival was 22.5 months in the digital intervention group versus 14.9 months in the control group.
Another app-based symptom reporting study at Memorial Sloan Kettering found a five-month extension of median overall survival among solid-tumor cancer patients, along with improvements in QoL during treatment. “One potential mechanism of action is early responsiveness to patient symptoms preventing adverse downstream consequences,” the researchers summarized.
Despite these early successes, organizations often must run clinical trials to reinforce the value of digital intervention to all stakeholders including not just regulators, doctors, and patients but also payers, who seek health economics data. DTx manufacturers are increasingly leaning into the decentralized clinical trial (DCT) model for its speed, efficiency, data quality, and patient-centric advantages.
Now a widely accepted trial model in the aftermath of the COVID-19 pandemic, DCTs use software to connect patients to trials. Travel to and from the trial site is minimized or eliminated; interaction with trial participants can be frequent (or, in cases where wearable medical devices are involved, it can be 24/7); and there are few geographic limitations, so participation can be more representative of the population.
In addition, there is a fundamental alignment between a DTx and a DCT. Since DTx is software rather than an oral or injectable formulation, there is no physical distribution or administering of medicines, just as there are often no physical sites in a DCT. There are no logistics: No shipping, storing, chain of control, cold storage, or biohazards; in addition, endpoints can be captured within the DTx application itself, making DCTs ideally suited for DTx studies. In the case of combination DTx/traditional studies in oncology, however, there will likely need to be some in-person site visits, so a “hybrid DCT” approach may be ideal.
Here are three key benefits of hybrid DCTs in oncology DTx development:
DCTs Boost Patient Recruitment, Retention, and Engagement
Patient retention and engagement have long been challenges in clinical research, but DCTs have had a uniquely positive impact on digital therapeutics studies. DCTs make participating in research easier and studies more accessible to participants who live far away from study centers or are unable to visit trial sites for various reasons. Without the need to perform all assessments at a clinical trial site, sponsors can successfully recruit patients from greatly expanded geographic areas. Opening studies up to more participants optimizes the patient pool and reduces the need to overenroll based on anticipated attrition or dropout rates.
Decentralization Improves Cost Efficiency
DCTs save costs, in part, by saving time. For instance, the single biggest time drain in drug clinical trials is patient recruitment, which can take about one-third or more of the duration of the entire trial and contributes to a trial’s high price tag. Similarly, recruiting a diverse patient population and keeping them engaged for DTx studies is draining. By expanding the geographic area for recruitment, DCTs speed recruitment across a more representative patient population. By removing many of the burdens associated with traditional trials, DCTs decrease dropout rates in DTx studies.
In addition to the financial benefit that comes from saving time, DCTs require less staffing and greatly reduce the need for sites and infrastructure. In fact, for many growing DTx companies, lengthy brick-and-mortar trials are unnecessary because they don’t have the same scope or needs as a randomized phase 2 or phase 3 study. The technology that DTx companies need to run a trial is materially different from the technology needed for a traditional drug trial. Further, much of the software needed for a DTx trial is already baked into the DTx app used in the study, so many of the components (such as EDC software) required for traditional clinical trials involving prescription drugs are not needed. This is not to suggest that a decentralized clinical trial is any less valid–just more innately streamlined. As a result, DTx companies can save substantially–reducing the costs by a factor of 20 or more–by picking just the technology needed rather than paying for complete functionality of an application or irrelevant bells and whistles.
This benefits the patient, too. Patients who use one app to complete all trial forms find participation much easier than using different devices or going into a site for repeat visits. Again, a better patient experience decreases study dropout rates and results in even greater savings and improved trial data.
Data Quality Improves with DCTs
DCTs enable DTx companies to collect real-world data directly from patients where they are most comfortable, minimizing the “white coat” effect, which has a quantifiable impact on data quality in the form of increased blood pressure in response to a clinician visit. Having a wider (more diverse) trial population means that the data collected are more reflective of real-world conditions; moreover, the potential for more precise data collection from patient interactions can translate into more granular data analysis. “Digital therapeutics are prescribed by a doctor often alongside a medicine, so it’s very reasonable to expect that we’ll see more DTx and drug combination regimens emerge in oncology in coming years,” concluded one top-10 pharmaceutical company’s digital health leader. “Combining innovative new treatments with evidence-based digital health solutions is one way we can think more holistically about cancer patient care to improve health outcomes.”
Invest in Technology, Profit in Better Health Outcomes
Improving preventative care and chronic disease management has helped slow the process of aging. In the United States, the 65 and older population has grown by over a third in the past decade, and the number of adults aged 85 and older is expected to nearly triple by 2060. Yet, living longer comes with risk. Genetic mutations are generally managed by the body’s ability to perform necessary repairs. However, with increasing age, the number of mutations also increases, which can give rise to cancer. Indeed, people aged 67 and older represent half of cancer patients and cancer is the second leading cause of death for people aged 85 and older. We owe it to ourselves to do something about this.
While the primary purpose of research is to learn, clinical research also seeks to advance treatments if possible. Many oncology patients, particularly those with aggressive disease, know that access to the most advanced medicines may entail being a part of a clinical trial. In comparison to other disease groups, cancer trials have the fewest age caps for enrollment. This is partly because, unlike chronological age or the number of years alive, physiological age (or how old one is due to genetics and lifestyle) is a better indicator of a patient’s ability to tolerate harsh treatment regimens and related toxicities. Older age is generally associated with reduced organ function and poorer performance status scores, which are risky for institutions ill-equipped to manage therapy-induced complications. Furthermore, sponsors would prefer to minimize instances of negative effects from their drugs; in response, many cancer clinical trials have an upper age limit of 70 to 80. Disappointingly, the median age of cancer participants enrolled in trials is an average of 6.49 years younger than that of patients with the same cancers not enrolled in trials. In essence, cancer patients who are granted entry to clinical trials are typically younger, fitter, and likelier to tolerate research regimens, while older, higher-risk patients are left without immediate access to potentially life-prolonging therapy. The very people who are most likely to require treatment with innovative therapies will not reap the benefits of a rigorous testing process.
Fortunately, these same patients are widely adopting technology: More than half of US adults age 65 and older own smartphones and 75% use the internet. Cancer patients are more likely to complete web-based questionnaires than paper-based forms. Oncology researchers often consider in-person follow-up essential to ensure safety and wellness in study participants. But this begs the question of whether the risk of missing an in-person observation outweighs the risk of transporting the infirm. Unless patients are so sick as to require hospitalization, are they not better off in the comfort of their homes, avoiding communicable infections for at least part of a trial’s duration?
One study shows that cancer patients who are offered the telehealth option improved communication with their providers, had 38% fewer hospital admissions and 31% fewer readmissions, and improved quality of life. This is significant because older cancer patients prefer quality of life over length of life. For cancer patients, untreated symptoms like gastrointestinal upset and pain can turn serious rapidly. Digital in-home symptom tracking tools for patients receiving chemotherapy offer pattern-recognition, severity detection, and real-time symptom management which reduce symptom burden by 43%, decrease the number of emergency room visits, and mitigate costs.
Advances in technology allow us to play 4-D video games, turn down our home’s heat while traveling in another state, and print objects from a personal-use device, yet we go about clinical research in an archaic fashion. Investment in our health is surely as important as investment in fun-to-haves, and yet trial participants remain too familiar with paper surveys, long clinic visits, and delayed responses to adverse events. If there is ever a time for clinical research to get up to speed with technology-driven industries, it’s now. And elderly cancer patients must be the focal point of this endeavor.
There are already pioneers committed to this mission. The Collaborations in Health, Aging, Research, and Technology (CHART) at the University of Illinois at Urbana-Champaign has constructed a research-focused “smart home” to learn how the elderly may benefit from using smart appliances, assistive robotics, and home sensors. Tools like these may seem like a luxury to some but could be essential for those who would otherwise rely on caregivers to meet basic health needs and achieve a sense of normalcy. If access to these tools improves someone’s ability to participate in a clinical trial–because they can now do just about anything a younger, healthier person can do, just differently–industry sponsors should pay attention. One cannot discount the cost of owning smart devices and tools. Insurance coverage and reimbursement programs could make a big difference in affordability. Traditional (less new) technology often carries the benefit of reduced or no cost for use. Examples include phone applications, wearable devices, and voice-operated mobile assistants.
It is important to note that some barriers to maximizing technology use in the elderly do exist. For instance, difficulty reading from small screens, manipulating voice-activated software, and understanding evolving terminology are a few. But these challenges are not insurmountable. Understanding how the elderly utilize technology is a step in the right direction. By engaging multidisciplinary research teams in rich discussions with patients and their caregivers, the potential for developing truly smart, customizable technology is vast. It may not be long before augmented reality glasses can be used for easily viewing and completing drug diaries as well as participating in virtual health visits. An automated call to a clinician when an in-dwelling catheter detects low levels of circulating red blood cells may be just around the corner. A bit of foresight, some creativity, and an incorporation of technology can allow investigators to spend more energy focusing on collecting and generating meaningful remote follow-up data that eventually improves treatment access and outcomes for elderly patients.
At present, we can only hope that our parents, grandparents, and even our future selves, if faced with cancer, will thrive in old age–not alone, but with the companionship of our aging loved ones. We can make this a reality by applying technology and thinking “outside of the (clinic) box” to bring our cancer clinical research to our elderly cancer patients.
Decentralized Trials Begin to Show Their Value in New Ways
The more experience clinical research professionals gain in conducting full or hybrid (onsite/offsite) decentralized clinical trials (DCTs), the more advantages beyond simple economics and convenience for patients they are realizing from the tactic, contributors to the next issue of ACRP’s Clinical Researcher journal suggest.
For example, in her forthcoming column on “Unique Considerations in Designing Decentralized Trials for Digital Therapeutics,” Pam Diamond, MD, cofounder and chief medical officer of Curavit Clinical Research, quotes an expert from the medical device arena as saying that DCTs can increase the quality of data by minimizing the Hawthorne Effect—where individuals modify an aspect of their behavior in response to their awareness of being observed. This phenomenon, also known as “white coat syndrome” in healthcare situations, is thought to be less of a factor when patients are in their home environment.
Diamond goes on to write that, “Fundamentally, a digital therapeutic (DTx) is software rather than a pill or injectable, so there is no distribution or administration of medicines. There are no physical logistics—no shipping, storing, chain of control, cold storage, or biohazards—plus endpoints can be captured within the DTx application itself, making DCTs ideally suited for DTx studies, whether the manufacturer’s goal is gaining regulatory approval or consumer and payer confidence.”
Meanwhile, in a column on “The Ecosystem of Decentralized Clinical Trials: It Takes a Village to Modernize Care,” MaryAnne Rizk, PhD, chief strategy officer for Medable, notes that, when “companies coordinate their efforts to design and execute DCTs, sponsors, investigators, and patients see the benefits. A connected ecosystem of DCT collaborators can streamline operations and data collection and resolve interoperability challenges. With a coordinated approach, the industry will accelerate this new model to make better medicines faster, safer, and more effective for every biology around the world.”
Rizk adds that, to navigate the new waters of DCT delivery, leading organizations are coming together to create a network of “best-of-breed, trial-enablement providers” that “includes contract research organizations, traditional and nontraditional investigator sites—including new retail pharmacy sites—and leading data and technology services providers” responsible for a range of trial support technologies and processes.
Still, Kristin Mauri, solutions services director for Remarque Systems, in her column on “DCTs: Key Considerations for Small-to-Midsized Biotech and Biopharma Companies,” looks at how the DCT trend may seem daunting for companies that feel that “the risks of treading this new territory—an area with complex data management demands and no clear regulatory guidance—outweigh the potential rewards.” However, Mauri adds that if some companies feel that DCTs are outside their comfort zone and budgets, that is not necessarily true.
As just one consideration, Mauri notes how, “untethered from sites, DCTs can recruit from anywhere, which often leads to faster enrollment and fewer screening failures. Further, that same geographic freedom also means fewer sites, thus fewer review boards, potentially lower regulatory costs, and greater flexibility around protocol amendments.”
Further, in his column on “A Hybrid Approach to Decentralized Clinical Trials,” Clincierge Cofounder and CEO Scott Gray writes that, “Moving forward, we must continue to assess the value provided by DCTs in ensuring patient experience and safety remain of the utmost priority. We should continue to build upon what has been learned since the onset of the pandemic. It is up to clinical trial stakeholders to determine the best approach for balancing the needs of patients and their caregivers against the goal of contract research organizations and pharmaceutical study sponsors. Whether that means a decentralized, traditional, or hybrid course, prioritizing clinical trial patients’ health and best interests ultimately encourages higher enrollment, increased retention, and more robust data collection results.”
The June 2022 issue of Clinical Researcher, with these columns and other content touching on DCTs and data analysis for trials, in addition to three peer-reviewed articles, will go online on or around June 21 on the ACRP website.
While digital therapeutics (DTx) companies are extremely optimistic about the promise of software-based interventions to prevent and treat diseases, they are still navigating unchartered territories around the best practices for clinical research, including patient recruitment and retention, quality of data, high costs, and uncertainty around regulatory guidelines.
At the same time, clinical trial models are rapidly evolving, adding further complexities. But one thing DTx companies do agree on is that the decentralized clinical trial (DCT) model is key to overcoming their biggest hurdles and improving the entire clinical research process.
A Patient-Centric Approach
Patient retention and engagement have long been challenges in clinical research, but DCTs have had a uniquely positive impact on DTx studies. DCTs make trials more accessible to participants who live far away from study centers. Opening studies up to more participants, optimizes the patient pool and reduces the need to over-enroll based on anticipated attrition or drop-out to improve cost efficiency.
Dr. Mike Aratow, Co-founder and Chief Medical Officer of Ellipsis Health, a DTx company that developed the first voice vital sign to quantify and manage depression and anxiety, explains, “A decentralized model not only aids patient recruitment because it removes many of the burdens associated with traditional trials, but it also makes it easier to reach underrepresented groups and those from a wider geographic landscape, providing real-world evidence and ecological validity. In traditional research, a significant amount of the medical data can’t be reproduced due to issues around patient retention and patient participation.”
Feel Therapeutics develops digital biomarkers and therapeutics for mental health using a proprietary wrist-worn wearable device. It monitors various physiological signals to extract insights on patients’ psychological and physical health. According to Feel CEO George Eleftheriou, “DCTs help optimize patient recruitment and improve engagement and retention. Wearable and digital technologies remotely measure endpoints while engaging participants in an unprecedented way and which naturally aligns with digital therapeutics that are intended to integrate into patients’ everyday lives. It is indicative that participants in our digital programs use our app for over 55 minutes per week.”
Reduced Costs
In 2020, Insider Intelligence predicted the global DTx market would hit $9 billion by 2025, but a year later sharply upped that forecast to $56 billion.1 Despite this market growth, the DTx industry is still in its infancy with most companies considered startups with modest resources. Cost efficiency is central to their success—and another reason why a DCT model complements the DTx business strategy.
DCTs save costs, in part, by saving time. For instance, the single biggest time drain in clinical trials is patient recruitment, which can take up to 30% to 40% of the duration of the entire trial process. By streamlining this process using digital tools and expanding the geographic area for recruitment, DCTs have faster recruitment, and require less staffing and infrastructure. DCTs allow researchers to customize DTx trials based on exact needs, patients, and commercialization strategy.
Additionally, the technology needed to run a DTx trial is materially different from the technology for traditional trials. Much of the software needed for a DTx trial is already baked into the DTx app being studied, so many of the robust components required for traditional clinical trials involving prescription drugs are not needed. DTx companies can save substantially—reducing the costs by a factor of 20 or more—by cherry-picking just the technology needed to run the DCT.
New data backs up the value of DCTs. According to a 2022 study by the Tufts Center for the Study of Drug Development, which compared published benchmarks on trial cycle times and costs with data from more than 150 DCTs conducted by trial software firm Medable, decentralized Phase 2 studies are completed one to three months faster than traditional trials and the time savings yield a net benefit that is up to five times greater than the upfront investment required. Decentralized Phase 3 trials with similar time savings yielded a net benefit that is up to 14 times greater the upfront investment.2
Improved Data Quality
Decentralized trials enable DTx companies to collect real-world data direct from patients where they are most comfortable, which has a quantifiable impact on data quality.
Dr. Erik Won, President and Chief Medical Officer of Wave Neuroscience, a DTx company that specializes in treating brain disorders, explained, “DCTs increase the quality of data by minimizing the Hawthorne Effect—a reactivity in which individuals modify an aspect of their behavior in response to their awareness of being observed, also known as ‘white coat syndrome’—because patients are in their home environment. With a decentralized trial, we get the best of both worlds. We can use other mechanisms to ensure that patients are following protocols while ensuring compliance. For instance, we record EEGs using wearables and ask patients to complete simple online surveys.”
DCTs also enable researchers to capture data and endpoints directly within the digital therapeutic itself for seamless data capture and less potential for “lost” information.
“DCTs enable us to collect passive, continuous, and objective data from users 24/7/365 and move from episodic patient-reported outcomes to continuous data collection,” added Feel’s Eleftheriou. “This rich data provides real-world evidence and allows us to explore novel biomarkers or digital endpoints in neuroscience and other chronic conditions with a high prevalence of mental health comorbidities, such as multiple sclerosis, certain cancers, and cardiac problems.”
Regulatory Approval
DTx companies operate in a nebulous regulatory environment, even as the Food and Drug Administration (FDA) works to clarify requirements. For example, the FDA has demonstrated its commitment to supporting digital health technologies recently through the publication of multiple relevant guidance documents as well as the founding of the Digital Health Center of Excellence (DHCoE) in the fall of 2020.
Yet, the regulatory landscape is complex, evolving quickly and differently in each country. Regulatory approval is not always required to go to market, disincentivizing studies. Many DTx manufacturers are left to make decisions on their own on whether they choose to seek regulatory approval, depending on their commercialization strategy and often take a bifurcated approach—seeking FDA approval for one variation of their product and not for another.
Wave Neurosciences follows FDA guidelines for conventional trials while making adaptations in non-FDA studies to maintain regulatory compliance. These “bridge” studies are often smaller, faster, less expensive and designed to gather enough validated data to determine if taking the next step to an FDA-approval study makes sense. In these cases, especially, a decentralized model makes it much easier and faster to stand up a “bridge” trial for DTx companies looking to determine what the next best steps should be for their product and commercialization strategy.
The Perfect Pairing
Fundamentally, DTx products are software, so there are no physical logistics—no shipping, storing, chain of control, cold storage, or biohazards plus endpoints can be captured directly within the DTx application, making DTx studies ideally suited for the digitally enabled decentralized model.
Even so, much is still to be learned in the emerging DTx market. While COVID may have forced researchers to lean into DCTs and the pandemic continues fueling a growing need for digital therapeutics, this perfect pairing will only benefit the industry and society a whole.
References:
1. Insider Intelligence, “DTx Trends and Companies to Watch in the Growing Digital Health Industry,” by Staff (July 29, 2021). See full resource here.
2. FierceBiotech, “Not Just for a Pandemic: DCTs Pay Off Financially, a Study Shows,” by Gareth Macdonald (January 12, 2022). See full resource here.
Despite rapid DCT evolution, there’s still room for progress: Curavit
A leader from the VCRO shares how far the industry has come with decentralized adoption, where opportunities for improvement exist, and what lies ahead.
While the pandemic knocked many clinical trial operations for a loop, the decentralized clinical trial (DCT) format has fueled a comeback since COVID-19’s arrival. Dave Hanaman (co-founder, president, and chief commercial officer of Curavit) spoke with Outsourcing-Pharma about progress made, lessons learned, and the road ahead.
OSP: How have decentralized trials evolved in the past two years?
DH: The biggest evolution has been the adoption of decentralized clinical trials (DCTs) by sponsors that would not have considered them without the catalyst of the pandemic. Before the pandemic, DCTs accounted for only 2-4% of trials and were projected to increase about 10% over the next 10 years. The pandemic and lockdowns forced the industry to get creative.
While there was a feeling early on that the use of DCTs might decline when the pandemic was over, the benefits of the model and the continued threats of new COVID variants proved otherwise. Now the DCT market’s estimated value is a staggering $1.63b USD by 2027, an annual growth rate of 14.8%, according to Precision Reports.
Much of this growth over the past six to 12 months is a result of the exploding digital therapeutics (DTx) market and their adoption of DCTs. According to Report Linker, the global DTx market is projected to reach $13.1b USD by 2026, up from $3.4b USD in 2021. These DTx companies are bringing novel software-based therapies and diagnostics into the market and their business and delivery models line up almost perfectly with DCTs because of the way these trials are designed from digital-first principles.
Gaining real-world results from a decentralized trial
When Lark Health decided to embark on its most recent decentralized trial with Curavit, a virtual CRO, its leaders saw the potential for a host of benefits.
According to OraLee Branch, the trial’s principal investigator and Lark’s director of clinical studies and research, a decentralized clinical trial (DCT) would be more patient-centric and convenient. It could boost efficiency, would likely be faster, and could help with recruiting a diverse population.
Lark joins an increasing amount of small to midsize companies now transitioning to DCTs, which provide solutions for a number of common logistical headaches.
It was also a natural fit for the midsize digital therapeutic company, which uses a cognitive behavioral therapy approach to create mobile apps aimed at managing and preventing chronic diseases, such as diabetes and hypertension. The apps’ features also include personalized coaching, and use artificial intelligence to help support lifestyle changes, such as weight loss, quitting smoking, or managing stress.
“I came to Lark from an academic background. I was a principal investigator and a full professor at various leading medical universities. So, I have a lot of experience in clinical trials and in managing decentralized, multi-site institutional trials,” Branch says.
For their upcoming study, which will test the use of a chronic disease prevention and management program, Lark wanted to enlist the help of other experts.
“We wanted a CRO who has had this kind of expertise, so that we can focus on what Lark does best, which is have great programs and great experiences for the user,” says Branch.
As an added bonus, they hope that having an outside CRO coordinating and managing data will bolster data integrity.
“We want this to be a high data integrity representation and the easiest way to do it is to have that external collection,” she says.
Here, Branch discusses how Lark plans to gain from using a DCT and how it is overcoming challenges associated with this approach.
PharmaVoice: What advantages do you hope decentralization will bring in terms of recruitment?
OraLee Branch: In conventional trials, which are typically brick and mortar or in-person trials, the people who end up participating are a select group. They are what you’d call a biased collection of participants. These are people who are willing and able to travel to the facility where the trial is conducted. People who join trials are sometimes more health conscious than the average person, or more likely to be from an urban versus a rural area. Participants also tend to be less diverse, or from different socioeconomic backgrounds than the general public. We want to remove that bias from the trial. That allows us to study people who are more likely to be the future users of Lark, so that the results that we’re obtaining are applicable to the general population. We want to make sure that we’re reaching the people who we know will be the users of our program.
Are there other benefits of a decentralized trial?
We are also hoping to connect a lot of fragmented information. We want to link laboratory results with clinical findings, and with the user’s every day well-being measures. That is why we really have our eyes on this decentralized clinical trial.
When Curavit Clinical Research launched in December 2019, the startup was looking to blaze a new trail in the clinical trial space. Quite simply, they added a “V” before the traditional “CRO,” and positioned themselves as the “first virtual contract research organization (VCRO).”
The timing could not have been more apt — or more of a challenge. The pandemic had supercharged the move toward decentralized clinical trials (DCTs), including virtual trials, and furthered already-strong regulatory tailwinds, Dave Hanaman, Curavit’s president and chief commercial officer, says. But it also created logistical challenges and upended the company’s planned roll-out strategy.
“We fully expected that the decentralized market, while small, was going to grow at a steady pace and a lot of that would come from Big Pharma,” Hanaman says.
But trials at large companies had suddenly come to a screeching halt.
“Big Pharma was suddenly working from home and if you weren’t doing COVID trials, but you were in clinical research, then you were sitting at home, and you were planning things for post-COVID,” Hanaman says.
Curavit pivoted quickly, focusing even more of its attention on small and midsize companies.
“Big Pharma has the luxury to be patient and that’s appropriate. Small, midsized biotech start-ups don’t,” he says. “They’ve got venture capital, they’ve got a binary equation on success. They’re either going to be successful or they’re not.”
Many early adopters of DCTs have historically been bigger companies, in large part because they have the resources to make the transition. But it’s actually smaller and midsize biotechs that stand to benefit disproportionately from decentralization, Hanaman says.
For these companies, DCTs have provided a lifeline to keep research moving.
An outsized benefit
For smaller pharma companies, DCTs can mitigate a number of challenges — from recruitment struggles to global deployment challenges. Decentralization can also help expedite trials, allowing them to adapt quickly in response to data.
Drugs and diagnostics at small to midsize companies typically target a focused, distinct audience, and often focus on rare diseases, Hanaman says.
“Decentralized trials allow them to recruit from all over the country or potentially all over the world,” Hanaman says.
Decentralized technology can also help facilitate global, multi-site trials, says Alison Holland, executive general manager, Digital and Decentralized Solutions for Medable, a software provider for decentralized trials.
“Very few companies, including the small to midsize, are working in just one jurisdiction,” Holland says. “They’re looking for broader exposure, broader registrations.”
According to Holland, decentralized trial providers can help to plan for site-specific needs, accommodating for local data collection, privacy, and regulatory requirements, which can vary by country.
DCT technologies and devices can also speed trials, allowing for more data collection in a shorter period of time, with greater efficiency and reach, Hanaman says. Researchers can then interpret this data more quickly and accurately, which can enhance patient safety, and encourage participation and participant satisfaction. For example, if a red flag is detected on a daily measure of blood pressure, heart rate, temperature or weight, the subject can be brought in for evaluation quickly.
DCTs also make trial participation more appealing because they require less hassle and travel to research sites. Easing the process helps to encourage those who might otherwise be reluctant to participate. This is particularly true for people who are in poor health, such as oncology patients.
“If home is a relaxing, safe environment for them, they might appreciate the option to be there,” Holland says.
Understanding the challenges
There are also some inherent challenges for small to midsize biotechs that chose to go the decentralized route. First, DCTs require an up-front investment, not only in terms of dollars, but of time, focus and energy, Hanaman explains. Making the leap ultimately enables these organizations to run more efficient trials going forward — but they have to get over that initial hurdle first.
Second, deviating from traditional research practices can bring risk and scrutiny.
“If everybody adopted DCT technologies and processes then everybody would start to benefit. But when one company does it, they expose themselves, correctly or incorrectly, to be challenged on their results,” Hanaman says.
For others, the main challenge is overcoming paralysis. Many companies are interested in DCTs, but simply don’t know where to start.
“It’s such an overwhelming thing,” Holland says, explaining that companies often don’t know how to adapt technology to their individual study.
For all of these reasons, many smaller organizations choose to dip a toe into the water rather than jump in all at once.
“A vast growing middle section of trials are hybrid, and that’s really where companies can and should be,” Hanaman says. “You don’t have to be all in on one or another. One can say, ‘What are the technologies that work for us? How do we design our trial from these digital first principles, and then add in traditional components in a way that is better for patients, better for research, better for outcomes?’ And that often is in this hybridized space.”
Strategies for successful implementation
In order for decentralization to work, it has to be implemented correctly. Some companies try to design a trial in a traditional way and then shoehorn in technology, Hanaman says. Instead of being more convenient for participants, the end result is a clunkier trial that increases the burden because participants still need to go to the site, but they also need to learn the technology.
Instead, companies should take a more comprehensive planning approach.
“I would encourage everyone to not to get overwhelmed by the breadth of what a DCT could be and to think about their protocol,” Holland says. “What’s the scientific question that their protocol is trying to answer?”
In particular, she advises that companies ask how they can answer that question in a more digital fashion, that allows for choices for the site and the patient.
Both Hanaman and Holland suggest consulting with DCT support providers as early as possible in the trial design process. This can help determine how technology can best be used to achieve trial aims. Ultimately, successful DCT adoption requires a focus on one core goal, Holland says.
“DCTs aren’t about no bricks and mortar, or no sites — it’s about amplifying the relationship between the site and the patient,” she says. “If we approach it from the perspective of ‘How do we engage patients with their clinicians and caregivers more?’ then it really opens up a huge opportunity for us to transform how we deliver healthcare and how we collect data.”
Oncology: Surprising Therapeutic Area Ripe for Decentralized Research
Given the complexity of cancer, some researchers are skeptical about the use of a decentralized clinical trial (DCT) model for oncology research. However, DCTs offer tremendous benefit, particularly in decreasing patient dropout rates and increasing patient engagement, two critical factors for oncology.
Oncology represents the largest research area globally, with 6.5% annual growth from 2000 to 2020 compared to 3.6% for nononcology drugs in development. At the same time, oncology trials face unique challenges including patient enrollment and retention problems, complex trial designs across more sites, larger data sets, longer durations, and more protocol deviations (to name only a few). In fact, the three phases of oncology trials last almost 12 years, on average, compared to 8 years for nononcology trials. And oncology trials generate a much higher volume of data: 3.1 million data points per protocol in phase 2 oncology compared with 1.9 million in nononcology.
It’s no surprise that, as of June 2021, only 5% of the 4,576 trials utilizing DCT strategies are oncology studies. Various explanations for this lag may include the type of investigational product, the need for invasive tests and scans, and the uncertainty surrounding the effect of remote assessments on data quality. However, a well-designed DCT that considers regulatory and operational concerns can not only overcome these issues but also improve research performance, data quality, and speed.
Wrong Assumption: Cancer Trial Patients Prefer In-Person Visits
Many cancer patients would prefer to stay home. For instance, patients diagnosed with acute myeloid leukemia—a cancer of the blood and bone marrow that progresses rapidly—juggle many physical and psychological side effects from the time they receive initial treatment through their post-hospitalization course. Prolonged symptom management, often involving nausea and fatigue, makes outpatient visits particularly challenging. Follow-up oncologist appointments are already time-consuming and may include blood transfusions, intravenous medication delivery, and comorbidity management. Tacking on additional research assessments before patients can go home may be more than they can bear.
DCT technologies enable remote monitoring so ailing cancer patients can remain in the comfort of their homes and reduce the burden of in-person visits, in turn, attracting more trial participants. Continuous remote monitoring provides the added benefit of better real-world data.
Pete, a middle-aged survivor of acute lymphoblastic leukemia, endured an arduous, three-year chemotherapy course. Three months into his treatment, he entered a clinical trial using blinatumomab, which was taken in parallel with his chemotherapy. Within just one month, his leukemia disappeared completely, but due to risk of recurrence, Pete underwent three more cycles of trial drug. Today, he sees considerable value in a DCT approach during the maintenance and monitoring phases, which will last for the next three years.
“I do televisits with my oncologist now, which is much easier,” said Pete in an interview for this article. “You can’t replace in-person visits in the early stages of a trial, but virtual technologies can ease the burden long-term.”
Digital Therapeutics Sector Projected to Grow Exponentially
As the digital therapeutics/software as a medical device sector continues its significant growth, clinical trials for the products are projected to expand logarithmically.
The space is seeing a big transformation from merely following patient symptoms to serving as interventions in a growing number of areas, according to Mark Opler, chief resource officer for directing research and development at WCG MedAvante-Prophase.
“This used to be, I would say, almost a fringe category of potential treatments. It’s moved considerably from symptom tracking to intervention,” Opler told CenterWatch Weekly. “There is an ever-widening array of conditions and symptoms that digital therapeutics are intended to treat. Mood disorders, particularly depression, anxiety, those have been traditionally thought of as the core target categories for digital therapeutics, but as time goes by, we’re seeing applications to psychosis, to trauma and to other diseases, including attention deficit and related conditions.”
The FDA has already approved a number of digital therapeutics products. These include Akili Interactive’s EndeavorRx, an ADHD videogame treatment for children, NightWare’s self-titled product that uses an AppleWatch and iPhone to disrupt nightmares without disturbing sleep and a trio of Pear Therapeutics apps for chronic insomnia, opioid use disorder and substance use disorder.
Digital therapeutics can also be developed to serve as coaching tools to help improve certain behaviors. While some are intended to serve as standalone products, others are being developed for use in combination with drugs or other medical devices. The sector’s growth is predicted to grow to $12.1 billion by 2026.
Because patients are using a piece of software, not simply taking a drug, determining what will be used as the placebo can be a taller order. Some companies come up with “inactive,” nontherapeutic software to serve as the placebo, while others develop games or use treatment as usual for patients in the placebo control group.
But according to Opler, it may be more fruitful to concede that this method of blinding “may be on some level challenging, if not impossible” and go another route: using an evaluator that has as few ties as possible to the trial beyond assessing patient symptoms, an avenue for blinding that’s gained greater traction in digital therapeutics trials.
“What’s transpired instead when you want to evaluate efficacy in an objective way in a digital therapeutics study is to have a fully independent and blinded evaluator, someone who is blinded as much as possible to the treatment and the study design, and whose only contact with the patient is evaluating their symptoms,” Opler said. “It’s tough to find the sugar pill equivalent in a digital therapeutics trial. Blinding the evaluator, keeping them independent from other aspects of conduct of the study, is another route to ensuring that the evidence we gather is rigorous and will be acceptable to the larger community.”
Endpoints are another big issue for digital therapeutics trials, according to Dave Hanaman, president and chief commercial officer of Curavit, a virtual CRO…
Curavit Earns HIPAA Seal of Compliance
January 10, 2022
BOSTON – January 5, 2022—Curavit Clinical Research announced today that it has taken all necessary steps to prove its good faith effort to achieve compliance with the Health Insurance Portability and Accountability Act (HIPAA). Through the use of Compliancy Group’s proprietary HIPAA solution, The Guard™, Curavit can track its compliance program and has earned its Seal of Compliance™.
The Seal of Compliance is issued to organizations that have implemented an effective HIPAA compliance program using The Guard. HIPAA is made up of a set of regulatory standards governing the security, privacy, and integrity of sensitive healthcare data called protected health information (PHI). PHI is any individually identifiable healthcare-related information. If vendors who service healthcare clients come into contact with PHI in any way, those vendors must be HIPAA compliant.
Curavit has completed Compliancy Group’s Implementation Program, adhering to the necessary regulatory standards outlined in the HIPAA Privacy Rule, Security Rule, Breach Notification Rule, Omnibus Rule, and HITECH. Compliancy Group has verified Curavit’s good faith effort to achieve HIPAA compliance through The Guard.
“HIPAA compliance is imperative for clinical research, increasingly soas the clinical trial model becomes more decentralized,” said Joel Morse, co-founder and CEO of Curavit. “As a virtual contract research organization that designs clinical trials from digital first principles, we take patient privacy very seriously, and have built our always–audit-readyplatform on validated technologies that support our HIPPA compliant processes.”
According to a statement by Compliancy Group, “Clients and patients are becoming more aware of HIPAA compliance requirements and how the regulation protects their personal information. Forward-thinking providers like Curavit choose the Seal of Compliance to differentiate their services.”
About Curavit
Curavit Clinical Research is a virtual contract research organization (VCRO) that designs and executes Decentralized Clinical Trials (DCTs) from digital first principles. Founded by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, minimizing the need for physical infrastructure and travel while increasing data quality and reducing patient burden. Curavit brings together the world’s leading researchers, enrolls previously underrepresented and underserved patient populations, and applies machine learning to health and social engagement information to recruit participants.For more information, visit www.curavitclinicalresearch.com.
Media Contact: Lisa Barbadora(610) 420-3413lbarbadora@barbadoraink.com
PM360 Presents the 2021 Innovators
December 13, 2021
Innovation. Transformation. Change. Adapt. These words and all their synonyms were repeated ad nauseum during these past two years as people, companies, organizations, and industries were forced to make drastic changes in the face of a global pandemic. As Rajiv Sodhi, COO, Microsoft India, said, “Innovation is no longer an option, but a necessity.” That was in relation to a Microsoft-IDC study in which 77% of businesses in India said that innovation is now a “must” for them to respond quickly to market challenges and opportunities.
Of course, this isn’t an issue isolated to just one country or one industry. According to BCG’s April 2021 report, “Overcoming the Innovation Readiness Gap,” 75% of the 1,500 global executives surveyed across all industries said that innovation is top-three priority at their company—a 10 percentage point increase from 2020, which is the largest year-over-year increase in the 15 years of BCG’s Most Innovative Companies survey. Furthermore, more than 60% of companies plan to boost investment in innovation, with one-third of them planning to do so significantly.
If these companies stick to their word, we may be entering a new age of innovation. That may be a sight to behold because in our industry alone, the innovations over the past two years have been significant. Yes, that includes COVID-19 vaccines developed in record time, but it’s more than that. Healthcare delivery, clinical trials, commercialization efforts, organization management, and much more were all reimagined to work better during a pandemic and even well into the future as we embrace our next normal.
For the past decade, our annual Innovations Issue has served as your guide to all things new and next in the industry to better prepare you for the future. As innovation only grows more crucial, so does this guide. From hundreds of submissions, we picked the most gamechanging innovations you need to know about in the following categories:
Companies (any organization developing new ways to push the industry forward)
Divisions (new sectors formed to address a particular problem facing the industry)
Startups (companies less than five years old pioneering new avenues in healthcare)
Products (software, apps, programs, and anything else designed to improve how those working in the industry do their jobs)
Services (compelling offerings that help the industry tackle new challenges)
Strategies (never-before-tried approaches that are changing how the industry operates)
These selections are meant to aide in your own innovation journey with potential partners, worthwhile offerings, and inspiring ideas that can help you stay ahead of the game in a world that has now made innovation one of its top priorities.
Advantages of Digital Decentralized Trials with Curavit’s Dave Hanaman | Interview
NEXT FRONTIER: The next frontier for clinical trials is in-silica research, also – confusingly – called virtual trials. In this future of research, “subjects” are computer models, data is real world data (RWD), and the experiments are conducted through computation – not human observation and measurement. There are already some good examples of this. The Economist recently reported on the one from the UK, but it will be a very long time before this is a significant disrupted to clinical research.
Curavit Clinical Research announced the appointments
Curavit Clinical Research announced the appointments of Jay Collier, as Chief Operating Officer, and Candice Del Rio, as Director of Clinical Operations.
Decentralized Clinical Trials: What Therapeutic Areas are Ripe for All-Virtual?
Before the pandemic, a December 2019 Industry Standard Research survey found that 38% of pharmaceutical sponsors and contract research organizations (CROs) expected virtual trials to be a major component of their portfolios, and 48% expected to run a trial with most activities conducted in participants’ homes. One year later when attendees at McKinsey’s Clinical Operations Roundtable were asked the same questions, the responses were 100% and 89%, respectively.
Today, most are asking what trials and what aspects of trials can be effectively decentralized and to what degree. Fully virtual or decentralized clinical trials (DCTs) typically handle all enrollment processes and assessments in a patient’s home, enabled by end-to-end digital tools and involve the self-administration of medicines. This model is gradually migrating from smaller, early-phase and post-approval studies toward larger pivotal trials, such as Otsuka and Click Therapeutics’ landmark fully remote clinical trial to investigate the effectiveness of digital therapeutics in reducing symptoms in adults diagnosed with major depressive disorder (announced in Feb 2021).
In the near term, sponsors, investigators, and CROs expect fully virtual trials to remain limited to a narrow set of use cases, such as a well-characterized drug with few adverse events in a mild indication, with end points suited to remote measurement. Long-term, however, fully virtual trials will be more widespread—especially in certain therapeutic areas such as rare disease, mental health, central nervous system, neurodegenerative and others that require patient populations that can’t physically travel or don’t live near a site.
Ultimately, the therapeutic area alone shouldn’t determine a trial design. Rather, each trial should be designed for-purpose and centered on patients. The target patient population, treatment, and indication will primarily determine whether a trial is fully virtual, hybrid or a traditional site-based trial. Even so, there are defining patient population characteristics in many therapeutic areas that can make some studies more likely candidates for all-virtual research.
Here are five therapeutic areas that are particularly apt for an all-virtual research approach, and that can serve as an entry point for hesitant sponsors interested in exploring this growing DCT model.
Diabetes—More than one in 10 Americans have diabetes and one in three or 88 million adults are prediabetic. Given the disease’s prevalence and its widespread geographic reach including many rural areas, diabetes is ripe for fully virtual research. Blood glucose values can be monitored continuously with wearable devices attached to the patient’s skin and automatically uploaded to a central platform in the cloud for easy access by trial investigators, sponsors, and the patients themselves.
In addition, the propensity of patients with Type two diabetes to be elderly or struggle with obesity can make it difficult for patients to travel to trial sites. These patients often have vascular problems which also can also hinder mobility. Further, diabetes is rampant in certain demographics such as Native Americans who are twice as likely to have diabetes as whites and often live in remote rural areas far away from the nearest clinician. Virtual trials bring lifesaving treatment to these patients and further the development of treatments that reflect the unique needs of a more representative population.
Cardiovascular—With wearable devices, including Apple watches, that monitor increasingly more sophisticated and wider range of cardiovascular endpoints remotely, research focused on cardiovascular diseases are apt for a fully virtual trial design. These devices accurately monitor and measure cardiac events and catch issues, such as atrial fibrillation (a common type of sustained cardiac arrhythmia) and ventricular tachycardia (abnormally fast heart rate) to alert the patient and remote physician in real time. Even some clothing items, such as bras, have sewn-in heart monitors! There are other devices that can be worn continuously for months at a time to capture more sophisticated measurements and automatically send data into the cloud. The same is true when it comes to managing blood pressure.
Like diabetes, cardiac patients are in all corners of the world and often many hours from central research sites and—due to their condition—may have mobility challenges and concerns. Virtual trials extend access to the millions living with heart disease and high blood pressure. Further, the data gained from continuous and multiple-symptom monitoring of cardiac patients is dramatically more useful in comparison to the less-reliable, one-hour, single-symptom testing completed at a site once a month or every few months. Heart arrhythmia often occurs only intermittently so it may not be picked up at the occasional site visit. Today’s wearable devices monitor blood pressure, heart rate and rhythm, and oxygen saturation levels as well as activity level (steps taken) so researchers can superimpose different measurements depending on what endpoint is being studied or combine multiple measurements for more meaningful information.
Central nervous system (CNS) diseases—Parkinson’s Disease, Multiple Sclerosis, Alzheimer’s disease, and other CNS diseases may dramatically impact patients’ mobility as well as hamper caregivers’ ability to bring affected loved ones to frequent clinician visits. All-virtual trials open these patients up to potential opportunities they might not otherwise ever have for a treatment.
Like cardiac wearable devices, there are an increasing number of new technologies that allow researchers to measure novel endpoints of patients in the comfort of their own homes and in more realistic life settings outside of a doctor’s office. Devices can continuously measure number of hand tremors per minute, for example, so a novel endpoint could be the reduction of hand tremors which was not as easily studied in traditional trials.
An electroencephalogram (EEG) is a widely used non-invasive method for monitoring the brain but has historically been a large and bulky technology, restricted to the monitoring of subjects in a lab or clinic while they are stationary. Today, we can use a wearable EEG, which overcomes these limitations and allows the long-term, non-invasive recording of brain signals at home.
Neuromuscular trials—Like patients with CNS disorders, patients struggling with neuromuscular diseases, including Duchene Muscular Dystrophy may have severe mobility challenges that make it difficult to make regular clinician visits. Fortunately, there are advanced activity monitors that do not interfere with movement on these patients such as ankle bracelets that can record various measurements continuously to, say, show how much activity a person takes part in over a period. Red Nucleus Clinical’s iTakeControl platform is a clinically approved solution that enables HIPAA-compliant video assessments of patients, live video research visits and audio recording to provide richer audio/visual data that is also auditable for compliance purposes.
Insights into Defining Decentralized Clinical Trials
Decentralized Clinical Trials (DCTs) have taken the main stage in the clinical trials industry, which was significantly facilitated during the pandemic. However, similar to the initiation of risk-based monitoring (RBM), the concept of DCTs is at an infancy stage, and many enterprises are competing to make their mark in the field. This prompted the formation of the Decentralized Trials & Research Alliance (DTRA) to help better define and advance DCTs. In this article, Dave Hanaman, Co-founder of Curavit, will discuss his perspectives on DCTs.
Moe Alsumidaie: What is a Virtual CRO (VCRO)?
Dave Hanaman: Co-founder Joel Morse and I conceived the company from our experience at C3i, where we spent 20 years at the intersection of digital technologies and clinical research. We saw this space evolving for years and wanted to disrupt research by positively applying technology in new ways. So we launched Curavit officially in November 2019 and became the first virtual CRO—a contract research organization dedicated exclusively to designing and executing decentralized clinical trials.
As a VCRO, Curavit runs fully decentralized trials from start to finish and acts as a virtual site, managing the decentralized components of a hybrid clinical trial. We leverage industry-leading digital technologies, devices, and our cloud-based DCT platform to centrally capture, aggregate, manage, and analyze trial data for sponsors. Curavit also brings specialized therapeutic expertise for decentralized trials to ensure the most proficient minds and the best technologies are applied to every research study.
As a VCRO, Curavit runs fully decentralized trials from start to finish and acts as a virtual site, managing the decentralized components of a hybrid clinical trial. We leverage industry-leading digital technologies, devices, and our cloud-based DCT platform to centrally capture, aggregate, manage, and analyze trial data for sponsors. Curavit also brings specialized therapeutic expertise for decentralized trials to ensure the most proficient minds and the best technologies are applied to every research study.
DH: Yes, and the technology is catching up to the vision. In 2007, Veeva introduced cloud-based CRM to an industry desperate for lower-cost technology models because so many major brand-name blockbuster drugs were coming off patent. Veeva’s well-touted success is an example of the right solution at the right time. Decentralized trials are similarly destined, supported by developments in IoT, wearables, and big data. People have been working to make DCT a reality for years, but the technology is finally maturing and readily available while the industry is calling for a greater focus on patients and access to trials for all. So once again, we have a case of the right solution at the right time.
MA:Are there concerns around data privacy and what precautions is Curavit taking to protect it, especially now where the U.S. and many Western nations are under attack by foreign hackers. What can be done to address those concerns using a DCT model for research?
DH: From banking to life sciences, every industry is extremely concerned about protecting data. As in most things, there are tradeoffs. Decentralized trials that do not involve sites can be an advantage in limiting data risk. DCTs can be much more secure in many ways because you can centralize data in very safe, modern cloud systems. That is what Curavit is doing.
Curavit’s platform has been purpose-built for decentralized trials with proven, industry-leading software. HIPAA compliance and validation are built into the individual tools as well as the overall platform. No corners were cut in terms of applying modern cyber defenses.
MA:Part of Curavit’s vision is to make research more accessible across all the demographics. How are you expanding clinical trials to those demographics through DCTs?
DH: First, DCT technologies and processes are fundamentally more suited to reaching previously underserved or underrepresented patient populations. It’s easier to expose more people to the opportunity to participate in research across social media, digital communities, and websites supporting specific diseases or conditions.
Second, and more specifically, DCTs leverage community-based outreach. For example, we partner with Clinispan out of North Carolina whose purpose is to recruit underserved populations. Par 80 in Boston partners with community health centers serving minority populations. These efforts reach out to minority populations to include those who distrust or have not been previously exposed to research.
Third, we have had ongoing discussions with a global pharmaceutical company interested in Native American populations that embody two distinct underserved groups: indigenous and rural populations.
MA:Where do you see DCTs going in the next ten years?
DH: Optimistically, in 10 years, we won’t think of DCTs as unusual because the technologies and processes will be commonplace. DCTs won’t be any more novel than computerized businesses are today.
Most data capture will be in the cloud a decade from now, and DCTs will enable a more burdenless patient research experience. To clarify, that doesn’t mean face-to-face interactions with physicians will go away. Even in complex therapeutic areas like oncology, there’s plenty of opportunities to use digital technologies to gather new data and reduce patient burden. We won’t think of DCTs as a distinct subset. In 2031, DCTs will have disrupted clinical research in profound ways that are better for all patients, better for all sponsors, and ultimately better for public health.
Decentralized Clinical Trials Poised to Expand Their Reach
An understanding of human nature suggests that in a post-COVID-19 era for clinical trials, the pendulum may temporarily swing away from the increased adoption of decentralized clinical trials (DCTs) and hybrid approaches that we’ve been witnessing and revert to something more closely resembling the traditional, in-person trial conduct practitioners and patients had been used to before 2020. However, Dave Hanaman, chief commercial officer for Curavait Clinical Research, sees “steep continued growth” in the years to come for new technologies and approaches that he believes can significantly advance the quality and reach of clinical trials.
“DCTs present a new opportunity to meet patients wherever they are,” says Hanaman. The approach they offer represents “an effective way to bring the trial to the patients,” he adds.
Acknowledging some industry “growing pains” as hybrid trials and DCTs have begun to take hold, Hanaman warns that some hybrid approaches are “the worst of both worlds,” with too heavy a physical footprint and overuse of technology.
However, Hanaman sees “strong levels of adoption” for hybrid trials in the next five to 10 years. “Much of the resistance has dropped,” he explains. “I think their use will be taken for granted” in the years to come, he says.
Hanaman is excited, too, about how hybrid trials and DCTs can expand the reach of clinical trials. In addition to traditionally underserved patient populations like African Americans and Hispanics, Hanaman notes the new technology and approach could improve trial access for native American and rural white populations. “Native American populations are often very far away from physical research sites,” he notes.
Further, internet coverage, long an obstacle to increased use of telehealth and DCTs, has improved in many of even the most geographically remote parts of the United States, Hanaman says.
DCTs and hybrid trials represent “a tremendous opportunity for patients and science,” he says. “I see so much more enthusiasm for [such approaches] to be included in trial design, and [they] will help us better reach the patients we’ve been missing.”
Meet The Disruptors: Dave Hanaman Of Curavit Clinical Research On The Three Things You Need To Shake Up Your Industry
As a part of our series about business leaders who are shaking things up in their industry, I had the pleasure of interviewing Dave Hanaman.
Dave Hanaman is co-founder, president and chief commercial officer of Curavit Clinical Research, a virtual contract research organization (VCRO), that designs and executes decentralized clinical trials (DCT). He is a proven entrepreneur, operator, and board director with successful, strategic exits to public companies. Founder of C3i, a Business Process Outsourcing (BPO) healthcare provider that was sold to a Fortune Global 500 company in 2018, Dave developed and led its sales, marketing, product development, and alliance strategies. Dave serves as a board member and advisor to several start-up and growth-stage companies in healthcare and technology. When not working, he enjoys spending time in the world’s mountains and oceans. He passes on his passion for the wilderness as an instructor for the National Outdoor Leadership School, where he teaches leadership to groups as diverse as the US Army, the US Forest Service, and Google. He graduated from the University of California at Berkeley and served as a deployed U.S. Navy intelligence officer.
Thank you so much for doing this with us! Before we dig in, our readers would like to get to know you a bit more. Can you tell us a bit about your “backstory”? What led you to this particular career path?
At my previous company, my co-founder, Joel Morse, and I spent 20 years at the intersection of clinical research and digital health technology, working with the world’s leading pharmaceutical companies. We became very interested in the ways that these technologies and processes could benefit patients, researchers, and healthcare organizations. I am very happy to be working with him and several other former colleagues now at Curavit, which launched in 2019.
Can you tell our readers what it is about the work you’re doing that’s disruptive?
At Curavit, we are designing and executing decentralized, or “virtual,” clinical trials, which are the application of digital technologies, wearable devices, internet-of-things, innovative trial design, and supportive regulation to increase the speed and fidelity of clinical research, while simultaneously attracting previously undeserved patient populations.
Can you share a story about the funniest mistake you made when you were first starting? Can you tell us what lesson you learned from that?
While not exactly a “funny” story, I have one that was completely unexpected. We announced Curavit at a major clinical research conference in January of 2020, when the industry was breathlessly predicting that 10% of all trials would be “virtual” in ten years. No one foresaw the impact of the pandemic and the unprecedented forced adoption of decentralized trials within months. We found ourselves suddenly accelerating toward our goals with massive tailwinds, but also buffeted by lots of noise and turbulence from the hype. We again learned the lesson that “the first casualty of battle is the plan,” and that you have to stay committed to the outcome while adapting to the things you can’t control.
We all need a little help along the journey. Who have been some of your mentors? Can you share a story about how they made an impact?
I learned so much from the men and women I served with in the Navy. From my Marine drill instructor, to the commanding officers I worked for, to my squadron mates and colleagues, they continue to inspire and motivate me every day. And of course my family; I have always enjoyed the full support of my wife and sons through the good, bad, and most of all uncertain times associated with being an entrepreneur.
In today’s parlance, being disruptive is usually a positive adjective. But is disrupting always good? When do we say the converse, that a system or structure has ‘withstood the test of time’? Can you articulate to our readers when disrupting an industry is positive, and when disrupting an industry is ‘not so positive’? Can you share some examples of what you mean?
I believe that “disruption” is a neutral word and that in practice it usually results in both positive and negative outcomes, depending on one’s perspective. For decentralized clinical trials (DCT), a good example might be the impact on sites. Are DCT’s “site-less” trials? Sometimes. Does that mean that some sites are negatively impacted by DCTs? Yes. But the flip-side of that may be reducing patient burden and increasing diverse enrollment, and those are positives. Furthermore, as with most disruption, it won’t be that simple. In this example, I believe some sites will prosper by embracing DCT technologies and processes, benefiting themselves as well as patients.
Can you share 3 of the best words of advice you’ve gotten along your journey? Please give a story or example for each.
One of our sales people once said, “If you’re explaining, you’re losing!” This means your value to your customers has to be clear and compelling.
An early advisor to my first company said, “Sometimes, you gotta tell ’em the baby is ugly.” In other words, don’t be afraid to see and speak the truth.
And recently, one of our current investors (and an advisor to our company) reminded me that my ultimate job is to detach and put myself in our customers’ shoes. Our success depends on our ability to meet and exceed customer needs and expectations over the long term.
We are sure you aren’t done. How are you going to shake things up next?
Curavit is my “next” right now. We are in our formative stage and are building out our team. We have an opportunity to do a lot of great work for the next few years and help shape the future of clinical research. That’s plenty for now, so no clear plans for a “next thing” just yet!
Do you have a book, podcast, or talk that’s had a deep impact on your thinking? Can you share a story with us? Can you explain why it was so resonant with you?
I usually read fiction or philosophy every night, even if only for a few minutes. In the gym or the car, I’ll listen to podcasts and audiobooks on a broad (and non-business-specific) array of topics often touching on history, exploration, geopolitics, and leadership. Right now I’m listening to the audio book “A Hunter Gatherer’s Guide to the 21st Century,” and just finished a 9/11 retrospective podcast series on Michael Morell’s Intelligence Matters podcast. Apropos of this interview, a keynote presentation that still resonates with me was one I heard years ago by Dr. Clayton Christensen on his seminal book, “The Innovator’s Dilemma.” That talk still informs my thinking around our strategy at Curavit today.
Can you please give us your favorite “Life Lesson Quote”? Can you share how that was relevant to you in your life?
I love quotes, and keep a list of my favorites. In this context, I’ll pick Theodore Roosevelt’s famous words found in “Man in the Arena.”
“It is not the critic who counts, not the man who points out how the strong man stumbles, or where the doer of deeds could have done them better. The credit belongs to the man in the arena, whose face is marred by dust and sweat and blood, who strives valiantly…who knows the great enthusiasms, the great devotions, who spends himself in a worthy cause, who at the best knows in the end the triumph of high achievement, and who at the worst, if he fails, at least fails while daring greatly, so that his place shall never be with those cold and timid souls who have never known neither victory nor defeat.” — Teddy Roosevelt
The most rewarding aspect of being an entrepreneur for me is commitment in the face of adversity and uncertainty which TR captures so well in that speech.
You are a person of great influence. If you could inspire a movement that would bring the most amount of good to the most amount of people, what would that be? You never know what your idea can trigger.
It would simply be to encourage people who are considering a different path to take the risk of engaging in a new venture. Of course we should plan and prepare, but eventually one simply has to make a leap of faith.
Curavit Clinical Research, a virtual contract research organization (VCRO) that designs and executes decentralized clinical trials (DCTs), announced today that it has joined the Decentralized Trials & Research Alliance (DTRA) to further the advancement and adoption of decentralized clinicals. Curavit Clinical Research has also announced the appointments of Jay Collier, as chief operating officer (COO), and Candice Del Rio, as director of clinical operations. The company also expanded its sales team with the hiring of Chris O’Shaughnessy, as vice president of business development, as well as Troy Hall and Bill Dreyer, as directors of business development. The expansion comes as DCTs continue their steady growth, punctuated by Curavit’s doubling its revenue since 2020.
Curavit joins decentralized trials group, predicts demand will keep growing
Curavit has joined the Decentralized Trials & Research Alliance, an industry-backed non-profit organization focused on the promotion of remote studies.
Membership of the group will see Curavit take part in the development of the fast growing the decentralized clinical trials market according to co-founder, president and chief commercial officer, Dave Hanaman.
“DTRA provides a broader platform for Curavit to discuss the innovations and research improvements that we are driving for our clients. Curavit will also have the benefit of collaborating with other innovators to solve new or emerging challenges in a way that is meaningful for the entire industry.”
Demand for decentralized trials has increased significantly in recent years – particularly since the pandemic – Hanaman told Clinical insider and predicted demand would continue.
“Curavit sees demand for DCTs daily in the form of customer feedback. Clients are developing long-term plans to leverage decentralized components in most of their trials. COVID-19 changed the industry’s approach, impacting everything from long-range planning to execution and it doesn’t seem like we are going back to traditional methods.”
He added, “Today, most trial designs have at least on decentralized component included and every large pharmaceutical company Curavit has spoken to over the last year has established a DCT group or team – often referenced as innovation team, trial optimization group, digital team or other similar nomenclature denoting DCTs.”
Curavit was established in 2020 in a bid to tap this growing section of the market. Last month the CRO expanded its sales team in a bid to broaden its service.
Hanaman said, “Curavit is a new company and establishing its sales force from scratch, so we need team members to support the demand. Prior, just Curavit founders have been managing client inquiries and working with clients to ensure long-term satisfaction and responsiveness.
“With our growth, that is not sustainable, as the Curavit leadership also need to devote time to helping to develop unique therapeutic-area-specific solutions for our clients.”
Image: Stock Photo Secrets
Beech Tree Labs Selects Curavit Clinical Research to Push Toward 100% Virtual Clinical Trials
Beech Tree Labs has developed a novel drug development platform known as resonant molecular signaling (RMS), that aims to address a wide range of illnesses by restoring normal cellular communications and correcting various imbalances triggering problems. The company opted to go virtual for their next Phase 2, FDA-authorized clinical trial to evaluate the effect of Beech Tree’s BT-TML therapy targeting COVID-19 patients. Although many companies have moved to at least some provisional virtual or hybrid approach during the pandemic, Beech Tree Labs took another step toward a permanent move to virtual trials by partnering with Curavit Clinical Research for a fully decentralized trial. The Park City, Utah-based venture has an ambitious plan to disrupt the operation of clinical trials, accelerating timelines and reducing cost while maintaining if not improving quality with improved, patient-centric care.
Move to Decentralized or Virtual Trials more than ‘Flipping a Switch’
Recently, TrialSite writer Joseph Constance assessed the emerging virtual clinical trials landscape particularly in the midst of the COVID-19 pandemic. In an earlier piece, Constance suggested the move to decent…
Chapel Hill startup targets seed funding after working to diversify Novavax Covid-19 vaccine trial
A Chapel Hill startup that helped bring diversity to Novavax’s (Nasdaq: NVAX) clinical trials for its Covid-19 vaccine is in the process of raising $250,000 in funding to help it continue to grow.
CliniSpan Health is actively raising seed funding to grow its team of eight to 20 by 2022, said Dezbee McDaniel, the company’s co-founder and head of business development who earned his undergraduate degree from UNC-Chapel Hill.
“We are looking to grow rapidly,” McDaniel said.
The company was started with the goal to bring more diversity to clinical trials, and in January the Novavax trial was the first CliniSpan began recruiting for, McDaniel said. About 17 percent of the Black participants at the Durham clinical trial site and 20 percent at the Chapel Hill site were referred to Novavax by CliniSpan, McDaniel said.
In 2020, the U.S. Food and Drug Administration approved 53 novel drugs that had clinical trials with a total of 32,000 patients. Of those patients, 75 percent were white, 8 percent were Black, 6 percent were Asian and 11 percent were Hispanic.
“We are heavily focused on African Americans right now,” McDaniel said. “We want to expand to groups who are Latinx, Native American, rural, women – a lot of other diverse groups who also need access to clinical trials.”
For now, the company is focusing on one population at a time, McDaniel said, because each group has a different history with the medical system and different preferences for how they want to be communicated with.
“With African Americans, the past mistreatment by the health care system is what we have to overcome and that’s something we haven’t directly affected, so it’s difficult to have that conversation sometimes,” McDaniel said.
Having people who reflect those groups do the outreach and recruitment helps make people more comfortable in participating, he said.
The transition to more decentralized trials also helps, McDaniel said.
“If people don’t have to show up physically and they can do it from home, then access for us becomes that much easier of a goal to achieve,” he said.
In addition to the Novavax trial, CliniSpan has partnered with Curavit, a fully virtual clinical trial organization, which perfectly complements CliniSpan’s infrastructure, McDaniel said.
CliniSpan has also signed a licensing agreement for its software with Capstone Health Alliance, a group purchasing organization for hospitals, he said.
“That’s something we’re trying to grow outside of our recruitment services,” McDaniel said. “We’re trying to help other diversity recruitment arms have technological infrastructure to carry out their processes more effectively.”
At the same time, CliniSpan will be helping to recruit for studies that its hospital network participates in, McDaniel said.
CliniSpan, which is led by founder and CEO Dr. David Lipsitz who did his residency at UNC-Chapel Hill, is currently working with five businesses in total and is generating revenue, though McDaniel did not disclose how much.
17 Virtual Clinical Trial Providers to Partner up With
Virtual clinical trial providers are your must-partners for any decentralized trial or contingency plan. In March 2020 the FDA encouraged sponsors to assess alternative methods for keeping their trials on track within the existing limitations under Covid-19 quarantine. Remote/virtual trials are no longer just a convenient way to shorten timelines and reduce costs but a rescue solution to ongoing clinical trials. From recruiting participants to designing their virtual experience, remote trial providers and technology can save your data and your budget.
Curavit Clinical Research, has been launched to help realise the potential of decentralised clinical trials
A new clinical trials company, Curavit Clinical Research, has been launched to help realise the potential of decentralised clinical trials.
Launched by industry veterans Joel Morse and Dave Hanaman, the new entity will focus on virtual trials.
Curavit Clinical Research co-founder and CEO Joel Morse said: “Curavit is the result of our desire to solve growing challenges to the important work of drug discovery.
“By combining experience, technology, and solid execution, we will bring cutting-edge research to previously untapped and underserved patient populations.”
Curavit Clinical Research is a next-generation clinical trial enterprise that provides decentralised clinical trial execution. It takes a clean-sheet approach to clinical trials, from the design phase to execution.
Optimised on a new virtual model, the company supports patients’ participation from wherever they live.
Curavit Clinical Research chief commercial officer and co-founder Dave Hanaman added: “We are fortunate to have worked with some of the most respected companies and visionary people in the life sciences industry, and are honored by the support we are receiving from them for this effort.”
Global clinical trials market stands at $70bn and continues to grow, while the success rate of trials continues to see a decline. This is often due to lack of enrollment by patients and participation from doctors.
Curavit Successfully Completes a Virtual Clinical Trial for Sana's Investigative Digital Therapeutic to Treat Symptoms of PTSD
Curavit Launches Health Economics and Outcomes Research (HEOR) Practice for Pharmaceutical Clinical Trials; Increasingly Critical for Digital Therapeutics
MedRhythms Selects Curavit as its Contract Research Organization (CRO) for a Chronic Stroke Decentralized Clinical Trial
Curavit Clinical Research Launches First Clinical Trial DEI Planning Toolkit
Curavit Clinical Research Appoints Jackie Kent to Board of Directors
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Digital Patient Recruitment Specialist Partners with Curavit Clinical Research to Speed Patient Enrollment in Decentralized Clinical Trials
ixlayer Partners with Curavit to Enable Convenient Patient Medical Testing Services for Decentralized Clinical Trials
Swing Therapeutics Selects Curavit to Provide Virtual Trial Site Services for Novel Digital Therapeutic Study for Fibromyalgia
Ripple Enterprise software to be deployed as part of the digital transformation in clinical trials spearheaded by Curavit
Curavit Named Runner up in BioUtah’s 2022 Entrepreneur & Investor Life Sciences Summit Pitch Competition
Curavit Earns HIPAA Seal of Compliance
Curavit Expands Leadership and Sales Teams to Drive Continued Growth of Decentralized Clinical Trials Across Life Sciences Industry
First All-Virtual CRO, Curavit, Joins the Decentralized Trials & Research Alliance
Beech Tree Labs selects Curavit Clinical Research for fully virtual COVID-19 clinical trial
Curavit Clinical Research and eMoyo USA, LLC Partner to Deliver High-Quality Home-Based Audiometric Data for Virtual Clinical Trials
Curavit Clinical Research officially launches with a focus on virtual trials
Curavit Successfully Completes a Virtual Clinical Trial for Sana’s Investigative Digital Therapeutic to Treat Symptoms of PTSD
Curavit Successfully Completes a Virtual Clinical Trial for Sana’s Investigative Digital Therapeutic to Treat Symptoms of PTSD
NEW YORK, Feb. 12, 2024 /PRNewswire/ — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), has successfully completed a decentralized trial for the Sana Device. Sana has submitted the trial data for Breakthrough Device Designation consideration from the U.S. Food and Drug Administration (FDA) for its wearable, virtual-reality-style mask that uses audiovisual stimulation to reduce symptoms of post-traumatic stress disorder (PTSD).
More than 45 patients were recruited from a Veteran’s hospital participated in the 28-day study. Curavit exceeded Sana’s expectations for participant retention with a 76% retention rate and managed all aspects of participation with remote-based clinical research coordinators (CRCs), a remote-based principal investigator, and fit-for-purpose technology platform including ePROs, eCOA, telehealth, device training, and randomization. Curavit CRCs captured participant experience with the Sana Device using industry-standard PHQ-9 survey and the Columbia Suicide Severity Risk Scale (C-SSRS) to capture levels of depression – all done remotely using electronic patient-reported outcomes assessments.
The Sana Device is a wearable device that aims to offer anxiety relief on-demand. The trial was carried out with a grant from CDMRP funds, disbursed through the Military Operational Medicine Research Program (part of the DoD). It was designed to gather evidence on the Device’s ability to allow patients suffering from PTSD to gain additional relief whilst on waiting lists for further specialty care.
“The Sana Device has tremendous potential to help patients with pain and mental health issues, but we needed a more efficient, modern way to study and demonstrate efficacy and safety,” explained Richard Hanbury, CEO of Sana Health. “In addition to gaining FDA approval, it is important for us to demonstrate the impact our device can have on healthcare economics so we can increase market access and get our innovation into the hands of more patients, faster. Curavit provided us with a streamlined path to capture real-world data with the utmost professionalism, allowing us to conduct a high-quality and successful trial. Thanks to Curavit, we are moving onto a larger pivotal study, funded by MOMRP (DoD).”
Curavit recently announced its Health Economics and Outcomes Research services to seamlessly capture evidence of the health economics value of novel pharmaceutical products, especially digital therapeutics. Curavit assesses the value and effect of medical interventions on both individual patients and population health levels of care, which can have an impact on market access post FDA approval.
“Real-world evidence is critical for DTx companies to achieve insurance coverage and reimbursement by demonstrating to payors and providers the full impact of these innovations. Curavit’s HEOR services produce the real-world data needed to unlock wider coverage and greater availability for transformative digital treatments,” added Andy Molnar, CEO of Digital Therapeutics Alliance (DTA).
“Sana Health’s origin story is emblematic of the company’s determination to bring innovative treatments to patients suffering from a range of disorders, and we are honored to help them along this journey,” concluded Joel Morse, CEO and co-founder of Curavit. “Our virtual site model with integrated HEOR data capture is key to helping companies like Sana reach both their scientific and commercial goals faster and give more patients alternative or complementary non-invasive treatment options.”
Learn more at SCOPE Summit (February 11-14, 2024) in Orlando, FL. To schedule a meeting, email media@curavit.io or stop by Curavit booth #832.
About Sana
Sana is anxiety relief and sleep on demand. Put comfortable sleep-mask style headset on, turn on, pulses of light and sound generate deep relaxation or sleep in ten minutes.
FDA Breakthrough Device Designation for Fibromyalgia, and pending for Neuropathic Pain and PTSD – based on incredibly strong clinical data. PTSD is DoD funded with DoD/VA trial near to completion. Expecting FDA approvals in 2024, with CMS coding and coverage under TCET. 50 million Americans can be helped by Sana.https://www.sana.io/bbc-video. Contact – enquiries@sana.io
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies that more effectively represent patient populations. For more, visit www.curavit.io.
Media Contacts:
Lisa Barbadora, +1 (610) 420-3413, lbarbadora@barbadoraink.com
Jamie Dabao Brown, +1 (626) 488-0732, jamie@barbadoraink.com
Curavit Launches Health Economics and Outcomes Research (HEOR) Practice for Pharmaceutical Clinical Trials; Increasingly Critical for Digital Therapeutics
Curavit Launches Health Economics and Outcomes Research (HEOR) Practice for Pharmaceutical Clinical Trials; Increasingly Critical for Digital Therapeutics
October 31, 2023
New offering captures evidence of health economics value of novel digital therapeutics to increase market access while reducing financial burden on the healthcare ecosystem
NEW YORK, Oct. 31, 2023 /PRNewswire/ — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), launches new Health Economics and Outcomes Research (HEOR) Practice. Curavit will incorporate HEOR services in clinical trials to capture evidence of the health economics value of novel pharmaceutical products, especially digital therapeutics which are striving to accelerate market momentum. Curavit will assess the value and effect of DTx interventions on both individual patients and population health levels of care.
Research shows that DTx products can drive better outcomes for patients living with chronic diseases – an area that experts predict will contribute to up to 84% of total global mortality by 2030. Additional studies show the potential of DTx products to improve health outcomes, reduce clinician workload, lower the costs of care, reduce health disparities based on geography or socioeconomic levels, and expand access to behavioral treatments for a range of conditions. However, getting these treatments to patients has been slow for various reasons – lack of clinician familiarity, administrative challenges, prescribing complications, and insufficient insurance coverage. Evidence that a DTx reduces economic impact can motivate government and private insurance coverage to pave the way for greater access.
“Real-world evidence is critical for DTx companies to achieve coverage and reimbursement by demonstrating to payors and providers the full impact of these innovations. Curavit’s HEOR services will produce the real-world data needed to unlock wider insurance coverage and availability for transformative digital treatments. Their decentralized trials rigorously demonstrating improved outcomes and reduced costs will be instrumental to driving comprehensive adoption of these breakthrough therapies,” said Andy Molnar, CEO of Digital Therapeutics Alliance (DTA).
MedRhythms, an early adopter, is working with Curavit to investigate long-term patient adherence, response durability, and healthcare economic value of its novel neurorehabilitation system to improve walking in adults with chronic stroke walking deficits. The study – known as OrcHESTRAS (Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation) – is a prospectively enrolled study, with a novel design that focuses on evidence generation and exploration of a product’s impact on reducing financial impact on the U.S. healthcare landscape.
“A cornerstone of our mission at MedRhythms is that our products must be accessible to patients. One way we do that is through furthering our evidence development,” said Owen McCarthy, President and co-Founder of MedRhythms. “In conjunction with clinical outcomes, HEOR assessments are an indispensable part of the evidence package needed to ‘speak the same language’ with payers and gain traction with a new prescription-only product.”
Curavit connected its Stratus platform to both claims and medical data networks, providing a single HIPAA-compliant environment for receiving, reviewing, and analyzing these data sets. When HEOR is part of the scope of a trial, Curavit’s clinical research coordinators confirm claims and medical data availability during the screening process to efficiently incorporate HEOR into the clinical trial. At study close-out, both HEOR and clinical data are then easily analyzed to quantify the financial impact of the therapeutic.
“Payers are concerned with health outcomes and cost-effectiveness, especially as healthcare costs keep rising and when it comes to less-understood digital therapeutics,” concluded Joel Morse, CEO and co-founder of Curavit. “We are helping DTx companies by seamlessly incorporating HEOR into their clinical trials, enabling them to not only capture safety and efficacy data but also financial data. The goal is that this information will prompt broader insurance coverage and use for patients in need. Digital medicines are here – let’s streamline the steps required to prescribe and implement them.”
Curavit and the Digital Therapeutics Alliance will be co-hosting educational events on November 3 in Boston, and December 7 in San Francisco. For more information on how to be part of these events, please email media@curavit.io.
About Digital Therapeutics Alliance As the leading global authority on the evolution of digital health technology, Digital Therapeutics Alliance (DTA) is a 501(c)(6) non-profit trade association of industry leaders and stakeholders dedicated to the understanding, adoption, and integration of digital therapeutics into healthcare. DTA works to enable expanded access to high quality, evidence-based digital therapeutics for patients, clinicians, and payors to improve clinical and health economic outcomes. As the leading international organization on digital therapeutic thought leadership and education, DTA provides the digital health ecosystem with the necessary tools to define, evaluate, and utilize DTx products.
About Curavit Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies that more effectively represent patient populations. For more, visit www.curavitclinicalresearch.com.
SOURCE Curavit Clinical Research
MedRhythms Selects Curavit as its Contract Research Organization (CRO) for a Chronic Stroke Decentralized Clinical Trial
MedRhythms Selects Curavit as its Contract Research Organization (CRO) for a Chronic Stroke Decentralized Clinical Trial
September 20, 2023
Curavit to research patient engagement, response durability, and health economics of MR-001, a medical devicethat aims to improve walking and ambulation in adults with chronic stroke
NEW YORK — September 20, 2023 — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), announced that it was selected as the VCRO for a study of MR-001, MedRhythms’ neurorehabilitation system designed to improve walking and ambulation in adults with chronic stroke walking deficits. The goal of the study is to further characterize the long-term economic and clinical benefits of MR-001 beyond what has been established in a multi-center, randomized clinical trial. This will also include evaluating patient engagement and response durability.
The study – known as OrcHESTRAS (Outcomes and Health Economics of Stroke using Rhythmic Auditory Stimulation) – is a prospectively enrolled study, with a novel design that focuses on evidence generation and exploration of a product’s impact on reducing financial impact on the U.S. healthcare landscape.
Curavit is responsible for managing all aspects of MedRhythms’ hybrid decentralized clinical trial (DCT) – from protocol finalization and Institutional Review Board (IRB) approvals to patient recruitment, testing at physical sites, remote site and patient monitoring and healthcare economics and outcomes analysis. The partnership between the companies began in June 2023, and the 12-month trial aims to enroll 225 participants by the end of the year.
“As innovators in healthcare, it’s essential to show that new technologies not only have the power to transform patients’ lives but are also economically prudent. Health economics research quantifies the long-term financial impact for patients, providers, and payers,” said Owen McCarthy, President and co-founder of MedRhythms. “Curavit’s tech-enabled approach to research lets us launch quickly while delivering a premier experience for everyone involved. As important, the study will be open to participants nearly nation-wide, thanks to Curavit’s virtual site solution, patient recruitment process, and smart strategies for collecting real-world healthcare economics data.”
MR-001 is based on Rhythmic Auditory Stimulation (RAS), a clinical intervention utilizing the mechanism of auditory-motor entrainment (“entrainment”). During entrainment, the motor and auditory systems in the brain subconsciously synchronize to an external auditory cue, such as music.
“We are honored to work with MedRhythms to manage such an important study of an innovative neurorehabilitation system to help stroke patients improve walking without invasive therapy or pills,” said Joel Morse, CEO and co-founder of Curavit. “We believe it is going to become increasingly important for DTx companies to capture health economics data to enable broader market access.”
Learn more at DTx East (September 26-28, 2023) where MedRhythms’ Owen McCarthy will be participating in a panel discussion “The Key Components of Building a Successful DTx product” on Sept., 26th at 12:30pm EST. To schedule a meeting, email media@curavit.io.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies that more effectively represent patient populations. For more, visit www.curavit.io.
Curavit Clinical Research Launches First Clinical Trial DEI Planning Toolkit
Virtual CRO operationalizes comprehensive service to help life sciences companies meet new federal guidelines for diversity, equity, and inclusion in clinical trials
June 20, 2023
NEW YORK — June 21, 2023 — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), announces its Inclusivity, Diversity, and Equity in Action (IDEA) toolkit. IDEA is a comprehensive clinical trial planning and support service designed to help clinical trial sponsors navigate the myriad challenges in developing and executing diversity action plans, now required by law for most clinical trials in the United States.
In April 2022, the FDA released draft guidance on improving enrollment for participants from underrepresented racial and ethnic populations in clinical trials. Now, Public Law 117-328 has taken the guidance a step further by requiring diversity action plans for clinical trials to determine drug and device safety and efficacy. The law, which incorporates the DEPICT Act, addresses decades of drug and device studies that enrolled primarily white men. This tendency has resulted in significant knowledge gaps on how treatments may affect a major portion of the population and perpetuated systemic health inequity. For example, in a 2020 study, enrollment of Black Americans in clinical trials was reported as 4.5% despite this group accounting for roughly 13% of the U.S. population and 22% of yearly cancer cases.
Curavit’s IDEA toolkit delivers support across five key functional areas:
Preliminary Situational Analysis – a summary document consisting of information about the trial’s specific patient population needs based on therapeutic area, disease risk factors, and potential obstacles to recruitment and retention. Curavit also helps sponsors create a plan to enroll appropriately representative numbers of participants from historically underrepresented populations to be submitted with investigational new drug (IND) and investigational device exemption (IDE) applications using templates informed by the most current FDA guidelines.
DEI Implementation Strategy – a streamlined trial execution strategy in alignment with the trial protocol and FDA diversity guidelines. Curavit provides recommendations for optimal patient recruitment methods, technologies, and partners; community/non-profit/patient advocacy partners; preferred site(s) or combination of alternative sites such as mobile units and home health networks; and tweaks to protocol designs to optimize patient enrollment and retention across historically underrepresented groups.
Content Review – feedback on the language, design, imagery, and cultural relevance of all recruitment marketing materials (i.e., websites, brochureware, social media posts, videos, advertising, and more). This is particularly relevant when engaging with populations from varying linguistic backgrounds and degrees of health literacy.
Continuous Check-Ins – data analytics displayed as near-real-time dashboards to track enrollment progress versus projected milestones to continuously monitor status. Curavit offers regular check-ins, too, to help ensure sponsors can pivot quickly to mediate a problem before going too far into the process. See sample dashboard here.
Ongoing Optimization – ongoing monitoring of patient participation throughout the life of the trial including real-time alerts to trial teams of spikes in patient dropouts and other urgent issues. Curavit will work with study teams to self-correct if faced with patient demographic concerns; even after meeting initial diversity enrollment goals and the trial is well underway.
“The life sciences industry must transform access to clinical trials so that we can bring novel therapeutics to all patients. We are motivated to produce the highest quality science, along with fairness and equity in clinical trials,” said Jackie Kent, an executive industry advisor and member of Curavit’s Board of Directors. “With its unique combination of insights, protocol development support, and planning guides, Curavit’s IDEA toolkit is helping companies turn lofty aspiration into action.”
Two early adopters of Curavit’s new service offering have leveraged planning templates to proactively ensure that they were familiar with the underrepresented patient populations that would be important to include in the trial, to compile effective strategies to recruit diverse groups of patients for enrollment, and to identify potential sites and investigators already engaged with the desired patient populations.
“Population representation in trials is a thorny problem to solve, especially for early-stage life sciences and digital therapeutics companies without major resources to invest – but for even larger companies, no one seems to know where to start,” said Joel Morse, CEO and co-founder of Curavit. “Curavit’s new IDEA service offers all companies the right scaffolding to architect a customized diversity strategy including the specialized expertise to efficiently execute that strategy.”
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies that more effectively represent patient populations. For more, visit www.curavitclinicalresearch.com.
Curavit Clinical Research Appoints Jackie Kent to Board of Directors
Calculate. Accommodate. Innovate.
February 6 – 9, 2023 | Orlando, FL
Industry’s first virtual CRO welcomes industry veteran to help guide its growth trajectory
NEW YORK — March 7, 2023 — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs) for digital therapeutics (DTx), announced the appointment of Jackie Kent to the Curavit Board of Directors. Ms. Kent is the first external fiduciary, independent life sciences industry veteran member on the Curavit Board.
With more than 30 years of experience in various technology and clinical research roles across the life sciences industry, Kent brings real-world knowledge to Curavit. She spent more than two decades at Eli Lilly and Company, including five years as Lilly’s TransCelerate BioPharma representative where she served in various capacities. Later, Kent accepted a position as head of product and then chief customer officer at Medidata. While at Medidata, Kent also served as vice Chairperson (2021) and chairperson (2022) of the Association of Clinical Research Organizations (ACRO).
Today, Kent is working independently to help drive change across the industry, focusing on the Society of Clinical Research Sites’ diversity program and sitting on various industry boards.
“Curavit is a rising star backed by brilliant leaders passionate about transforming research using innovative technologies and services, and I’m honored to be part of their continued trajectory,” said Kent. “We are at an inflection point where all the good intentions, wishful thinking, and blood, sweat, and tears is yielding real change. It’s the pinnacle of my three+ decades of effort to offer my knowledge, experience, and insights to innovators like Curavit and take leaps forward in clinical research.”
With the new appointment, the Curavit Board will consist of five directors. Kent’s appointment comes just three months after Curavit announced a Series A funding round of $5 million to accelerate its growing portfolio of research in the global DTx market (projected to grow at a CAGR of 31.4% through 2026). The round brings Curavit’s total capital raised to more than $8 million. The funding is being used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription DTx trials.
“Curavit is focused on building a leading, sustainable company in the clinical research industry and needs expertise from both our internal management team and independent experts outside of our organization, said Joel Morse, co-founder and CEO of Curavit. “Jackie brings tremendous value with rich and well-rounded experience across big pharma, tech, and at the site level. She has a deep understanding of clinical trial operations from sponsor, site, and software perspectives.”
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visit www.curavitclinicalresearch.com.
Curavit Raises $5 Million in Series A Funding to Accelerate Growth in Digital Therapeutics Clinical Research
Industry’s first virtual CRO that specializes in decentralized clinical trials achieves key milestones
November 14, 2022
PHILADELPHIA and NEW YORK — Nov. 14, 2022 — Curavit Clinical Research, a virtual contract research organization (VCRO) that specializes in decentralized clinical trials (DCTs), today announced it raised $5 million in Series A funding to accelerate its growing portfolio of research in the global digital therapeutics (DTx) market (projected to grow at a CAGR of 31.4% through 2026). The new funding will be used to expand the company’s DCT capabilities, partnerships, and market adoption of Curavit’s virtual CRO services and platform for prescription and non-prescription digital therapeutics trials.
The funding was led by early-stage technology investor Osage Venture Partners with additional investment from Royal Street Ventures and Narrow Gauge Ventures. It adds to early investments from Curavit founders and individual investors, including industry veterans Clark Golestani, former president of emerging businesses and global CIO of Merck, and former president and co-founder of Veeva Systems, Matt Wallach.
“In order to dramatically lower the cost and increase the speed of clinical trials, the industry must take a new, digital-first approach,” said Wallach who serves on Curavit’s board of advisors. “Curavit was founded by seasoned veterans with deep experience in that sweet spot where technology innovation meets process excellence so I’m proud to play a part in their journey to improve clinical trials.”
“This is an important milestone for Curavit and the industry’s continued momentum in digital therapeutics and decentralized approaches to clinical research,” said Joel Morse, co-founder and CEO of Curavit. “Traditional trial processes and timelines are insufficient – and they limit patient participation. New digital therapeutics are ideally suited for a DCT approach and will help improve access and drive new unique therapies to patients faster.”
The funding brings Curavit’s total capital raised to more than $8 million. Curavit has more than doubled its revenue in 2020 and 2021 and is on the same pace this year. More than half of its customer base are emerging digital therapeutics companies whose clinical research needs align with Curavit’s focus on virtual site services and DCT expertise.
“We are pleased to partner with Curavit on the next phase of their journey,” said Nate Lentz, Managing Partner at Osage Venture Partners. “The COVID-19 pandemic and rapid growth of digital therapeutics has driven a new digital model, where clinical trials are increasingly decentralized and require a new combination of technologies, services, and expertise not available in the marketplace. Curavit’s team and offering are well-positioned to fill this void and become the leading virtual CRO.”
Since its founding in late 2019, Curavit has accomplished key successes on its mission to bring clinical trials of innovative therapies to more patients in the cloud, including:
Support for important research with digital therapeutics companies, including Swing Therapeutics, Lark Health, Curio, and Sana.
Strategic partnerships with life sciences digital technology and data providers, including Ripple Science, for its direct-to-patient software platform; ixlayer, to provide easy access to clinical-grade diagnostic lab testing in DCTs; and 1nHealth, for digital patient recruitment and enrollment.
Hired experienced industry leaders in top positions including Jay Collier as COO, Candice Del Rio as director of clinical operations, and Chris O’Shaughnessy as VP of business development.In other news, Curavit joined the Digital Therapeutics Alliance, whose aim is to broaden the understanding, adoption, and integration of clinically evaluated digital therapeutics with patients, clinicians, payors, policymakers through education, advocacy, and cross-industry collaboration.
About Osage Ventures
Osage Venture Partners (OVP) is a venture capital firm located just outside of Philadelphia, PA. It partners with exceptional entrepreneurs, building the next generation of leading B2B software and tech-enabled services companies. OVP has consistently focused on this strategy since its inception in 2005, making over sixty investments in early-stage B2B companies over that time. For more information, visit OsageVenturePartners.com.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visit www.curavitclinicalresearch.com.
Media Contacts:
Lisa Barbadora, +1 (610) 420-3413, lbarbadora@barbadoraink.com
Jamie Dabao Brown, +1 (626) 488-0732, jamie@barbadoraink.com
BOSTON — Sept. 6, 2022 —Curavit Clinical Research, a virtual contract research organization (VCRO), has entered into a long-term partnership with ixlayer to provide easy access to clinical-grade diagnostic lab testing for decentralized clinical trials (DCTs). ixlayer seamlessly integrates with Curavit’s platform and makes health testing fast and convenient for patients, improving trial enrollment completion rates. Curavit and ixlayer’s first collaboration is for Swing Therapeutics’ trial of an investigational digital therapeutic (DTx) for fibromyalgia.
ixlayer’s patient-centric lab testing program offers multiple testing formats, including flexible digital options, and thousands of testing combinations. The company offers multi-modality sample selection options, such as at-home self-collect, at-home collection assisted (i.e., mobile phlebotomy), and sample collection at a local patient service center. By making health testing easy for patients, Curavit and ixlayer help sponsor organizations improve completion rates and likelihood of patient retention the duration of the trial so organizations get the data they need to facilitate breakthrough discoveries and bring life-changing healthcare innovation to market quickly.
“Curavit is driving innovation in hybrid and decentralized clinical trials, and we are proud to be part of their mission,” said Pouria Sanae, CEO and co-founder of ixlayer. “Lab testing is an integral part of most clinical trials but can burden patients in traditional settings. At ixlayer, we reduce friction for patients and sponsors by digitally simplifying the process and streamlining data collection on the back end.”
Curavit will remotely recruit, screen, consent, and enroll at least 80 participants in Swing’s PROSPER-FM trial and leverage ixlayer’s platform to streamline clinical urine tests to determine participant eligibility. During televisit screening, Curavit’s clinical coordinators seamlessly schedule the patient’s test at one of more than 2,000 conveniently located lab sites in the U.S. through Curavit’s virtual site platform. ixlayer manages all administrative needs, including payment and curating lab results, unburdening patients, resulting in a more positive early-trial experience.
“ixlayer is the leader in flexible lab and home-based testing services,” said Joel Morse, co-founder and CEO of Curavit. “By partnering with ixlayer, we are setting the foundation for a frictionless patient experience in our decentralized clinical trials and greater trial accessibility. As important, together we are improving the efficiency of trials to get important new therapies to more patients faster.”
To learn more about how ixlayer and Curavit are innovating to drive decentralized clinical trials into the mainstream, see us in Boston at DPharm 2022 (Sept. 13-14, 2022) – booth #26.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visit www.curavitclinicalresearch.com.
About ixlayer
ixlayer is redefining next-generation consumer experiences for lab testing and better health outcomes.
Retailers, health plans, employers, government entities, and health systems chose ixlayer because our solutions allows them to run health testing programs under their own brand at scale. The ixlayer solution includes an extensive test menu, over 1000 testing options, and omnichannel marketing to end users. ixlayer’s lab independent platform powers health testing programs for partners including the United States Coast Guard, Stanford Health, Salesforce, three of the eight largest national health plans in the US and one of the top retail pharmacy chains. Visit www.ixlayer.com.
Digital Patient Recruitment Specialist Partners with Curavit Clinical Research to Speed Patient Enrollment in Decentralized Clinical Trials
1nHealth and Curavit surpass expectations by nearly 3x, enrolling 50 patients in Lark DTx trial in 10 days
October 4, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON, Oct. 4, 2022 /PRNewswire/ —Curavit Clinical Research, a virtual contract research organization (VCRO), announced that it is partnering with1nHealth, a patient recruitment provider, to speed patient recruitment digitally for decentralized clinical trials (DCTs). 1nHealth integrates with Curavit’sDCT platform, speeding trial enrollment and improving retention. Curavit and 1nHealth’s first collaboration is for Lark Health’s trial of an investigational digital therapeutic (DTx) for chronic cardiovascular disease.
Lark’s Heart Health program is designed to help patients manage cardiovascular disease (CVD) risk factors and reduce the rate of future cardiovascular diseases or events. The smartphone-based program uses conversational AI, connected devices, and remote patient monitoring to activate and engage patients by addressing CVD risk factors such as diet, exercise, and tobacco use.
“We are excited to partner with Curavit to improve patient recruitment by simplifying participant identification and enrollment through digital channels,” said Dan Brenner, founder and CEO of 1nHealth. “As a technology-first company, we are closely aligned with Curavit’s mission to bring trials to patients in the cloud. Our partnership will drive faster enrollments and more inclusive trial participation.”
Through targeted ads on key digital media channels (i.e., Google, Reddit, Facebook, Instagram), 1nHealth recruited qualified patients for Lark’s Heart Health trial, surpassing sponsor expectations. In addition, nearly 40% of patients who clicked on an ad went on to complete the pre-screen form. Beyond the early successful 10-day enrollment drive, Curavit and 1nHealth have successfully recruited, consented, and enrolled a total of 150 patients in impressive time.
“During the initial phase of our Heart Health program, we heavily relied on our ability to engage with the right patient, at the right time – not only to track progress but also to ensure the greatest impact on each participant,” said Dr. OraLee Branch, director of clinical studies at Lark Health. “Curavit and 1nHealth’s innovative methods of engaging patients helped us reach our goal. Plus, their fast patient enrollment supports our mission to help patients predisposed to a life-threatening condition or illness.”
Patient recruitment has been a long-time challenge for clinical trials. Globally,90% clinical trials are delayed due to insufficient patient enrollment. As a result, timelines are typically extended to nearly double their original duration to meet desired enrollment levels. In contrast, 1nHealth enrolls 90% of trials on time using highly targeted, all-digital methods. Together, Curavit and 1nHealth are working to overcome recruitment challenges and help usher in the next generation of decentralized clinical trials.
“COVID-19 initially forced the life sciences industry to try a decentralized approach, and now the indisputable success of DCTs will drive the industry to make it the norm for the foreseeable future,” said Dave Hanaman, co-founder and chief commercial officer at Curavit. “Industry vanguards like 1nHealth bring the kind of innovative tools and thinking that will help speed new therapies to more patients. It’s exciting.”
Lark’s Heart Health program will be commercially available in early Q1 2023. To learn more about Lark and its suite of chronic condition prevention and management programs, please visit them online atwww.lark.com.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visitwww.curavitclinicalresearch.com.
About 1nHealth
1nHealth fills studies faster by using novel methodologies to deliver high-performing ads across all digital channels. 1nHealth uses AI to help find patients who are simply being missed by other recruitment vendors. 1nHealth works with top CROs, Pharma companies and most of the leading DCT providers, as well as across 40+ TAs, delivering full enrollment for site-based, hybrid, and fully decentralized studies. Visit www.1nhealth.com.
ixlayer Partners with Curavit to Enable Convenient Patient Medical Testing Services for Decentralized Clinical Trials
September 6, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON — Sept. 6, 2022 —Curavit Clinical Research, a virtual contract research organization (VCRO), has entered into a long-term partnership with ixlayer to provide easy access to clinical-grade diagnostic lab testing for decentralized clinical trials (DCTs). ixlayer seamlessly integrates with Curavit’s platform and makes health testing fast and convenient for patients, improving trial enrollment completion rates. Curavit and ixlayer’s first collaboration is for Swing Therapeutics’ trial of an investigational digital therapeutic (DTx) for fibromyalgia.
ixlayer’s patient-centric lab testing program offers multiple testing formats, including flexible digital options, and thousands of testing combinations. The company offers multi-modality sample selection options, such as at-home self-collect, at-home collection assisted (i.e., mobile phlebotomy), and sample collection at a local patient service center. By making health testing easy for patients, Curavit and ixlayer help sponsor organizations improve completion rates and likelihood of patient retention the duration of the trial so organizations get the data they need to facilitate breakthrough discoveries and bring life-changing healthcare innovation to market quickly.
“Curavit is driving innovation in hybrid and decentralized clinical trials, and we are proud to be part of their mission,” said Pouria Sanae, CEO and co-founder of ixlayer. “Lab testing is an integral part of most clinical trials but can burden patients in traditional settings. At ixlayer, we reduce friction for patients and sponsors by digitally simplifying the process and streamlining data collection on the back end.”
Curavit will remotely recruit, screen, consent, and enroll at least 80 participants in Swing’s PROSPER-FM trial and leverage ixlayer’s platform to streamline clinical urine tests to determine participant eligibility. During televisit screening, Curavit’s clinical coordinators seamlessly schedule the patient’s test at one of more than 2,000 conveniently located lab sites in the U.S. through Curavit’s virtual site platform. ixlayer manages all administrative needs, including payment and curating lab results, unburdening patients, resulting in a more positive early-trial experience.
“ixlayer is the leader in flexible lab and home-based testing services,” said Joel Morse, co-founder and CEO of Curavit. “By partnering with ixlayer, we are setting the foundation for a frictionless patient experience in our decentralized clinical trials and greater trial accessibility. As important, together we are improving the efficiency of trials to get important new therapies to more patients faster.”
To learn more about how ixlayer and Curavit are innovating to drive decentralized clinical trials into the mainstream, see us in Boston at DPharm 2022 (Sept. 13-14, 2022) – booth #26.
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, ultimately bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visit www.curavitclinicalresearch.com.
About ixlayer
ixlayer is redefining next-generation consumer experiences for lab testing and better health outcomes.
Retailers, health plans, employers, government entities, and health systems chose ixlayer because our solutions allows them to run health testing programs under their own brand at scale. The ixlayer solution includes an extensive test menu, over 1000 testing options, and omnichannel marketing to end users. ixlayer’s lab independent platform powers health testing programs for partners including the United States Coast Guard, Stanford Health, Salesforce, three of the eight largest national health plans in the US and one of the top retail pharmacy chains. Visit www.ixlayer.com.
Swing Therapeutics Selects Curavit to Provide Virtual Trial Site Services for Novel Digital Therapeutic Study for Fibromyalgia
June 28, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON, June 28, 2022 /PRNewswire/ — Curavit Clinical Research, a virtual contract research organization (VCRO), has been selected by digital therapeutics company, Swing Therapeutics, to be a virtual site for its pivotal trial of an investigational digital therapeutic (DTx) for fibromyalgia. Curavit will remotely recruit, screen, consent, and enroll participants in Swing’s PROSPER-FM randomized clinical trial from across the United States. Curavit will then manage participants throughout the 12-week clinical trial. By eliminating physical and geographic barriers to trial participation and execution, Curavit can scale quickly and improve patient enrollment by at least 10x over a traditional trial, speeding trial execution.
Fibromyalgia is a chronic and debilitating pain condition that affects more than 10 million Americans. It is characterized by widespread musculoskeletal pain often accompanied by fatigue, sleep, memory, and mood disruptions. Swing developed its digital therapeutic with the goal of providing an accessible behavioral therapy option that can be used alongside medication, physical therapy, and other standard-of-care treatments.
“We are focused on getting patient recruitment right,” said Mike Rosenbluth, PhD, Chief Executive Officer at Swing, which recently announced a $10M Series A funding round. “Curavit’s virtual services model enables us to efficiently recruit participants representative of the entire patient population. It solves a huge challenge and will be critical to rapidly develop the evidence needed to bring an effective digital therapy to millions suffering from chronic illness.”
Swing marks Curavit’s 10th DTx client signed in less than six months, a trend in line with a booming global DTx market projected to hit $13.1 billion by 2026, up from $3.4 billion in 2021. Curavit’s decentralized clinical trial (DCT) expertise makes the company well-suited to support prescription and non-prescription DTx studies. Fundamentally, there are no physical logistics with a DTx – no shipping, storing, chain of control, cold storage, or biohazards, plus endpoints can often be captured within the DTx application itself, naturally aligning DCTs with DTx studies.
“Swing is committed to developing scientifically backed digital treatments and evidence to clinically validate their use in the real world, making representative patient participation critical,” said Joel Morse, co-founder and CEO of Curavit. “Our operational model prioritizes patient recruitment and removes geographic boundaries to expand the pool without the expense of physical infrastructure. With zero physical site visits, too, patients are less burdened and more likely to stick with the trial the duration.”
About Curavit
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, and bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across representative populations. Visit www.curavitclinicalresearch.com.
SOURCE Curavit Clinical Research
Ripple Enterprise software to be deployed as part of the digital transformation in clinical trials spearheaded by Curavit
April 12, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
ANN ARBOR, MI- April 12, 2022 – Ripple Science, a digital clinical trial software company, today announced a partnership with Curavit Clinical Research (Curavit) to deploy Ripple Recruit, the company’s newly expanded enterprise software platform, to support several digital therapeutic decentralized clinical trials. Ripple is a natural fit for Curavit’s digital-first disruptive approach to engaging patients, conducting research, and accelerating time to market of new discoveries, especially in the exploding field of digital therapeutics.
“We are hyper-focused on the unique needs of DTx manufacturers, with nearly half of our rapidly growing customer base running studies on novel digital therapeutics,” said Joel Morse, CEO of Curavit, the industry’s first virtual CRO. “Ripple Recruit offers scalable, patient-centric functionality that aligns with our decentralized clinical trial service offering for emerging DTx companies.”
Ripple Enterprise is the world’s only direct-to-patient software platform designed to support decentralized, virtual, and hybrid clinical trials. Designed and audited to 21 CFR Part 11, HIPAA, GDPR and SOC2 standards, Ripple Enterprise enables the entire clinical trial industry to adopt digital clinical trial workflows driving down costs and expanding access to a more diverse pool of patients.
“We’re excited to partner with Curavit which is on the cutting edge of the digital transformation in clinical trials,” said Peter Falzon, CEO of Ripple Science. “This partnership is our largest contract to date and validates our strategic decision to invest in Ripple Enterprise as a response to customer demand for DCT enabling software at enterprise scale.”
About Curavit:
Curavit Clinical Research is a full-service, virtual contract research organization (VCRO), focused on designing and executing digital-first decentralized clinical trials (DCTs). Founded in 2020 by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, bringing trials to patients in the cloud. Curavit’s digital-first DCTs improve timelines, reduce costs, yield real-world data, and increase patient access for therapies more effective across diverse populations. For more information, visit www.curavitclinicalresearch.com.
About Ripple Science:
Ripple Science, a clinical trial technology company, is leading the digital transformation in clinical trials with a direct-to-patient software platform that was built by researchers for researchers. By improving the user experience, increasing regulatory compliance, and further connecting the ecosystem through digital innovation and technology, Ripple delivers real-time transparency, game-changing efficiencies, and more secure workflows & data sharing, concerning all aspects of patient engagement from first contact to last patient visit, whether virtual or in-person.
Ripple Science was named a Top 50 Company to Watch in 2021 by Michigan Celebrates Small Businesses and recognized in 2022 by Purpose Jobs and Cronicle Tech News as one of the fastest growing health tech startup companies in Ann Arbor.
Media Contacts:
Curavit:
Lisa Barbadora
Barbadora INK
lbarbadora@barbadoraink.com / 610-420-3413
Ripple Science:
Anna Falzon
Curavit Named Runner up in BioUtah’s 2022 Entrepreneur & Investor Life Sciences Summit Pitch Competition
April 7, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
SALT LAKE CITY, April 6, 2022 — Curavit Clinical Research, the first virtual contract research organization (VCRO), announced that it was recently named runner up in the 2022 Wilson Sonsini Entrepreneur & Investor Life Sciences Summit (E&I Summit) pitch competition, sponsored by Morgan Stanley. Curavit received the award for its innovative business model and ‘digital first’ approach to democratizing clinical research.
Now in its 7th year, the E&I Summit, presented by BioUtah, BioHive and the PIVOT Center, attracted a record setting 300+ registrants, along with an impressive line-up of distinguished speakers, national and local investors, and numerous Utah life sciences startups.
“We are so happy to be recognized in this capacity by our industry peers and to have had the opportunity to share what we are doing at Curavit,” said Dave Hanaman, Co-founder, President and Chief Commercial Officer of Curavit. “It was an honor to be able to share the stage with so many inspiring companies. Our satisfaction of being recognized by the judges was only overshadowed by the exciting ability to engage with so many innovative entrepreneurs and investors in the dynamic Utah ecosystem.”
The conference featured notable keynote speakers, including Jake Manoukian, Head of Investment Strategy for JP Morgan, who shared insights on market trends and life sciences investment, and Stanford University professor Matt Vassar, who provided a thought-provoking address on “Telling Your Story.”
Out of a total of 21 life sciences companies, Curavit advanced to the popular Pitch Track session through a competitive selection process and went on to win second place after Eliksa Therapeutics.
For being named runner-up in the competition, Curavit was refunded its $1,000 registration fee, which the company donated to BioHive, an organization launched last year to brand, build and bring together the life sciences and healthcare innovation industry in Utah. The funds will be used to support local underrepresented communities, aligned with industry partners to promote K-12 STEM education, workforce development and awareness.
“We are thrilled Curavit sees the value in what we’re doing at BioHive to tell the story of our industry and unite all of the stakeholders for life sciences and healthcare innovation in Utah,” said Katelin Roberts, Executive Director at BioHive. “Their organization works at the nexus of patients, research and industry. Similarly, BioHive seeks to be the hub for our community, and their donation will go toward building our state into a premier life sciences and healthcare innovation ecosystem.”
About Curavit
Curavit Clinical Research is a Virtual Contract Resource Organization (VCRO) that designs and executes Decentralized Clinical Trials (DCT) from digital first principles. Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, eliminating the need for physical infrastructure and travel while increasing data quality. Curavit brings together the world’s leading researchers, enrolls previously underserved patient populations, and applies machine learning to health and social engagement information to recruit participants. The company’s cloud-based, central virtual site is always audit ready. For more, visit www.curavitclinicalresearch.com
About BioUtah
BioUtah is an independent 501(c)(6) trade association serving Utah’s life sciences industry. Its member companies reflect a broad spectrum of the industry with strengths in medical device manufacturing and services, research and testing, biotechnology, biopharmaceuticals, advanced diagnostics, and healthIT, amongst others; and are a key driver of Utah’s economy and life-saving treatments and cures for patients. BioHive is a chartered organization of BioUtah. Its mission is to brand, build and bring together Utah’s life sciences and healthcare innovation community. For more, visit https://bioutah.org/.
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON – January 5, 2022—Curavit Clinical Research announced today that it has taken all necessary steps to prove its good faith effort to achieve compliance with the Health Insurance Portability and Accountability Act (HIPAA). Through the use of Compliancy Group’s proprietary HIPAA solution, The Guard™, Curavit can track its compliance program and has earned its Seal of Compliance™.
The Seal of Compliance is issued to organizations that have implemented an effective HIPAA compliance program using The Guard. HIPAA is made up of a set of regulatory standards governing the security, privacy, and integrity of sensitive healthcare data called protected health information (PHI). PHI is any individually identifiable healthcare-related information. If vendors who service healthcare clients come into contact with PHI in any way, those vendors must be HIPAA compliant.
Curavit has completed Compliancy Group’s Implementation Program, adhering to the necessary regulatory standards outlined in the HIPAA Privacy Rule, Security Rule, Breach Notification Rule, Omnibus Rule, and HITECH. Compliancy Group has verified Curavit’s good faith effort to achieve HIPAA compliance through The Guard.
“HIPAA compliance is imperative for clinical research, increasingly soas the clinical trial model becomes more decentralized,” said Joel Morse, co-founder and CEO of Curavit. “As a virtual contract research organization that designs clinical trials from digital first principles, we take patient privacy very seriously, and have built our always–audit-readyplatform on validated technologies that support our HIPPA compliant processes.”
According to a statement by Compliancy Group, “Clients and patients are becoming more aware of HIPAA compliance requirements and how the regulation protects their personal information. Forward-thinking providers like Curavit choose the Seal of Compliance to differentiate their services.”
About Curavit
Curavit Clinical Research is a virtual contract research organization (VCRO) that designs and executes Decentralized Clinical Trials (DCTs) from digital first principles. Founded by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, minimizing the need for physical infrastructure and travel while increasing data quality and reducing patient burden. Curavit brings together the world’s leading researchers, enrolls previously underrepresented and underserved patient populations, and applies machine learning to health and social engagement information to recruit participants.For more information, visit www.curavitclinicalresearch.com.
Media Contact: Lisa Barbadora(610) 420-3413lbarbadora@barbadoraink.com
Curavit Expands Leadership and Sales Teams to Drive Continued Growth of Decentralized Clinical Trials Across Life Sciences Industry
September 29, 2021
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON— Sept.29, 2021 — Curavit Clinical Research, a virtual contract research organization (VCRO) that designs and executes decentralized clinical trials (DCTs), announced today the appointments of Jay Collier, as chief operating officer (COO), and Candice Del Rio, as director of clinical operations. The company also expanded its sales team with the hiring of industry veterans, Chris O’Shaughnessy, as vice president of business development, as well as Troy Hall and Bill Dreyer, as directors of business development. The expansion comes as DCTs continue their steady growth, punctuated by Curavit’s doubling its revenue since 2020.
Curavit continues to disrupt clinical research by enabling digitally native DCTs that expand trial access to previously underserved patients while improving patient participation, data quality, and research speed.
Jay Collier brings more than 20 years of operational experience serving global clients in life sciences and clinical research. In his role as COO, he will manage all aspects of service delivery for Curavit’s clients. Prior to joining Curavit, Collier served in various leadership positions, most recently senior vice president of U.S. operations at C3i Solutions, a global leader in healthcare technology services. C3i was also founded by Curavit’s co-founders, Joel Morse and Dave Hannaman, who sold the company to a Fortune Global 500 company in 2018. Before C3i, Collier served in various director-level roles at Nextel.
“Having worked with Joel and Dave for nearly 20 years at their previous company, I’m excited to join Curavit to help build another successful venture that will streamline the clinical trial process with advanced technology, and essentially improve global health and save lives,” said Collier. “This is a huge opportunity to make a meaningful difference in clinical research for years to come.”
Candice Del Rio, Curavit’s new director of clinical operations, has more than 12 years of clinical research experience in academic , clinical, and industry settings. Prior to joining Curavit, she worked at Massachusetts General Hospital as a clinical research nurse and an oncology/hematology nurse for over a decade. She will bring her in-depth experience in the areas of clinical trial development, patient recruitment and retention, and process improvement to manage projects and ensure customer success.
In addition, Curavit welcomes Chris O’Shaughnessy, as vice president of business development, who also comes from C3i Solutions; Bill Dreyer, as director of business development, previously manager of business development for EPL Archives, Inc.; and Troy Hall, as director of business development, who last served as a cardiovascular institutional specialist at Johnson & Johnson.
“It’s an exciting time at Curavit as we grow along with the rapid evolution and adoption of decentralized clinical research,” said Joel Morse, co-founder and CEO of Curavit. “We are taking it to the next level and our new team members will bring their collective expertise to help drive innovation and customer satisfaction, while delivering our scalable and purpose built clinical trial platform to our clients.”
Curavit Clinical Research is a virtual contract research organization (VCRO) that designs and executes Decentralized Clinical Trials (DCTs). Founded by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, minimizing the need for physical infrastructure and travel while increasing data quality. Curavit brings together the world’s leading researchers, enrolls previously untapped and underserved patient populations, and applies machine learning to health and social engagement information to recruit participants. Current clients include Frequency Therapeutics, Beech Tree Laboratories, Brown University, and Boston Medical Center. For more information, visit www.curavitclinicalresearch.com.
First All-Virtual CRO, Curavit, Joins the Decentralized Trials & Research Alliance
September 29, 2021
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
BOSTON— Sept. 29, 2021 — Curavit Clinical Research, a virtual contract research organization (VCRO) that designs and executes decentralized clinical trials (DCTs), announced today that it has joined the Decentralized Trial & Research Alliance (DTRA) to further the advancement and adoption of decentralized clinicals.
Established in 2020, the DTRA enables collaboration of stakeholders to accelerate the adoption of patient-focused, decentralized clinical trials and research within life sciences and healthcare through education and research. It works to make research participation accessible to everyone, enabled by the consistent, widespread adoption of appropriate decentralized research methods.
“We are extremely gratified to welcome Curavit to the ‘Decentralized Trials & Research Alliance,’ said Amir Kalali, MD, founder of several collaborative life science communities, and co-Chair of DTRA. “By advancing decentralized research we can make the clinical trial process more patient-focused, increase trial efficiency and encourage use of technologies. We are excited by Curavit’s commitment to embracing decentralized trials and to changing the culture that has been the rate limiter to innovation.”
“This is an important opportunity for Curavit to collaborate with other DCT pioneers to further our mutual mission of making patient participation more accessible across all demographics,” said Joel Morse, co-founder and CEO of Curavit. “We look forward to sharing best practices, research methodologies, and technologies that will transform how research gets done.”
Curavit Clinical Research is a virtual contract research organization (VCRO) that designs and executes Decentralized Clinical Trials (DCTs). Founded by experts with decades of experience in technology and clinical research, Curavit leverages emerging technologies in digital health, cloud computing, and data science to recruit, engage, and monitor diverse patient populations without borders, minimizing the need for physical infrastructure and travel while increasing data quality. Curavit brings together the world’s leading researchers, enrolls previously untapped and underserved patient populations, and applies machine learning to health and social engagement information to recruit participants. Current clients include Frequency Therapeutics, Beech Tree Laboratories, Brown University, and Boston Medical Center. For more information, visit www.curavitclinicalresearch.com.
Beech Tree Labs selects Curavit Clinical Research for fully virtual COVID-19 clinical trial
September 18, 2022
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
Curavit chosen for expertise in decentralized trial design and execution.
Beechtree Labs has chosen Curavit Clinical Research for a fully decentralized clinical trial to investigate a promising Covid-19 therapy. The FDA-authorized phase 2 clinical study will evaluate the effect of Beech Tree’s BTL-TML therapy on mean duration and severity of disease in 40 outpatients aged 60 years or older with underlying conditions. The study also assesses the safety of BTL-TML over 10 days of treatment and an additional four days of follow-up.
The trial is unique in that it is a fully decentralized clinical trial, made possible by applying virtual trial design protocols, digital telehealth technologies, electronic patient reported outcomes (ePRO), and full web and contact center patient support to eliminate the need for in-person office visits.
Thomas Hatch, Director of Business Development at Beech Tree said: “We chose Curavit because of their exclusive focus on designing and executing virtual trials. We needed a company with Curavit’s expertise in this important new discipline of clinical research in order to make this trial possible.” Joel Morse, CEO of Curavit added: “This is a unique opportunity to apply modern trial design and telehealth
technologies to allow patients to participate in this study without the potential risk of traveling to physical sites and to participate from the safety and comfort of their own homes.”
ABOUT CURAVIT
Curavit is a new type of clinical research company that designs and executes decentralized – also called “virtual” – clinical trials. Curavit brings together the world’s leading researchers, enrolls previously untapped and underserved patient populations, applies machine learning algorithms to health and social
engagement information, and leverages leading telehealth, patient data platform, and medical device technologies. Connect: https://www.linkedin.com/company/curavit/
Follow: https://twitter.com/CuravitClinical
ABOUT BEECHTREE LABS
Located in Providence, RI, Beech Tree Labs, Inc. (BTL) focuses on the discovery and early development of therapeutic agents that address a spectrum of unmet medical needs. The company has an extensive portfolio of patented formulations for products intended to treat such disorders as urinary incontinence, allergies, benign prostatic hypertrophy, anxiety, chronic obstructive pulmonary disease and herpesvirus infections. BTL has conducted over 15 FDA- authorized phase 2 trials and has out-licensed both technology and products.
LEARN MORE ABOUT THIS STUDY
The current FDA-approved Phase II pilot study is taking place in Draper, Utah at Intermountain Clinical Research. Additional sites will open in the future. To learn more about this study:
● You or your doctor may contact the study research staff ( deann@icrtrials.com ) or call
833-358-3784.
● Visit the study website: https://www.sickwithcoronavirus.com/
● You can also visit clinicaltrials.gov, the U.S. National Library of Medicine database of clinical studies conducted around the world. ClinicalTrials.gov identifier (NCT number): NCT04522830
Curavit Clinical Research and eMoyo USA, LLC Partner to Deliver High-Quality Home-Based Audiometric Data for Virtual Clinical Trials
September 9, 2020
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
New solution allows patients to participate in clinical trials from the comfort and safety of their own homes.
Curavit Clinical Research, a virtual research organization, and eMoyo USA, LLC, the USA representative of eMoyo, a global leader in healthcare technology, today
announced a partnership to pave the way for hearing research studies to continue
during the COVID-19 pandemic. Curavit’s virtual team of audiologists remotely monitor the hearing of research subjects in their homes using the eMoyo KUDUwave™ Pro boothless audiometer. This portable, high-frequency audiometer enables a booth-free operation and extended high frequency hearing test up to 16 kHz, making the KUDUwave™ Pro the ideal solution for virtual or hybrid clinical trials which require audiology end points.
“With KUDUwave™ boothless diagnostic audiometers we can now test patients in their homes without compromising on the quality of testing and without having to transport and maintain an audiometric booth. Given COVID-19, this provides a lower health risk for the study subjects, as the soundbooth could be a source of cross contamination.” says Grant Talbot, of eMoyo.
Prior to every planned audiology test date, a Curavit Study Team member sends a
pre-configured laptop and a KUDUwave headset to each study subject’s home. Working directly with the study subject, a Curavit audiologist initiates a telemedicine visit where they perform a thorough, high quality audiometric evaluation. The final data is securely transferred to the Curavit Study Team, where it is stored in a secure and validated system.
“With this unique technology, teamwork, and our proprietary protocols, a clinical trial subject performs a comprehensive hearing test in less than an hour, all from the comfort of their home,” said Dr. Pam Diamond, Otolaryngologist, co-founder and Chief Medical Officer of Curavit. “KUDUwave combines the audiometer, headset and required components into a single, portable, lightweight device weighing only half a pound and it is controlled remotely by our audiologists using a laptop and telemedicine software. This process may shorten the trial timeline, and minimizes the potential for trial disruption due to COVID-19.”
“We are honored to partner with eMoyo and to work together to bring these
best-in-class offerings to virtual and hybrid clinical trials. Though catalyzed by the
coronavirus pandemic, this solution makes participation in these types of trials far easier for many more patients, regardless of where they live, work and study; thus ensuring richer data and better research outcomes well into the future.” says Dave Hanaman, Chief Commercial Officer and co-founder of Curavit.
About Curavit Clinical Research
Curavit is a new type of clinical research company that designs and executes decentralized – also called “virtual” trials. Curavit brings together the world’s leading researchers, enrolls previously untapped and underserved patient populations, applies machine learning algorithms to health and social engagement information, and leverages leading telehealth, patient data platform, and medical device technologies. https://curavit.io/
About eMoyo
eMoyo is a team of passionate designers, engineers, clinicians and dreamers working to make the world a better place, by creating the technology that gives the world access to quality healthcare. This includes advocating for policy change, health implementation science and the development of technology that empowers healthcare providers to reach further and do more. Founded by Dr Dirk Koekemoer, eMoyo is an ISO13485 company renowned for producing high quality, innovative technology and services. https://emoyo.net/
Curavit Clinical Research officially launches with a focus on virtual trials
February 18, 2020
There’s more than one way to architect a decentralized clinical trial (DCT). While this flexible model has many benefits, it can be overwhelming to bring together all the right elements to operationalize a trial that’s predominantly digital. Every trial is unique, so it is not realistic to templatize (impose a standard implementation template on) a DCT. But four common, fundamental components combine to facilitate a seamless, patient-centric DCT.
“It’s like a trial in a box, but each box is a little bit different,” said Steve Rosenberg, CEO of a cloud-based platform company that powers decentralized clinical trials. Even with a DCT’s inherent optionality, foundational components can ease implementation and improve execution.
Industry veterans Joel Morse and Dave Hanaman announce the formation of a company to lead into the future of clinical trials.
Curavit was founded to help realize the potential of decentralized trials. Mssrs. Morse and Hanaman come to Curavit with over twenty five years of experience, founding, building, and running successful technology-enabled healthcare companies. https://curavit.io/about
● The $70 billion global clinical trials market continues to grow , while the success rate of trials continues to decline, often due to lack of enrollment and participation by patients and doctors.
● New technologies and new approaches offer an opportunity to both increase success rates and decrease the costs of traditional clinical trials.
● Virtual clinical trials take advantage of these trends and opportunities.
● Just a small percentage of trials today, virtual trials are projected to increase geometrically due to their advantages.
“Curavit is the result of our desire to solve growing challenges to the important work of drug discovery.” said Joel Morse , Chief Executive Officer and Co-Founder of Curavit. “By combining experience, technology, and solid execution, we will bring cutting-edge research to previously untapped and underserved patient populations.” Chief Commercial Officer and Co-Founder Dave Hanaman added:
“We are fortunate to have worked with some of the most respected companies and visionary people in the life sciences industry, and are honored by the support we are receiving from them for this effort.”
ABOUT CURAVIT
Curavit Clinical Research takes a clean sheet approach to clinical trial design and execution. Optimized on a new “virtual” – or decentralized – model, the company supports patients’ participation from wherever they live, across the country, and around the globe. Curavit teams with distinguished principal investigators in specific therapeutic classes, works from archetypal investigational sites in major research hubs, leverages best-in-class industry standard patient data platforms and mobile health devices to collect, manage and protect patient data. By applying advanced data analytic algorithms to patient information and real world evidence, Curavit partners with healthcare entities to identify, qualify, and enroll patients in approved clinical trials. Curavit plans to open its first site in Boston this summer.
Connect: https://www.linkedin.com/company/curavit/
Follow: https://twitter.com/CuravitClinical




















































































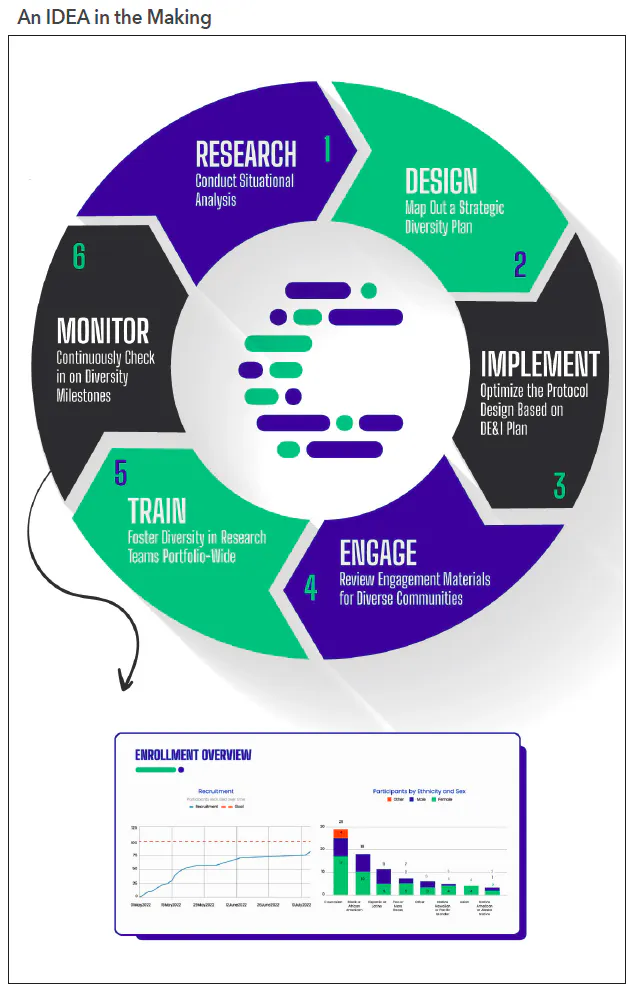


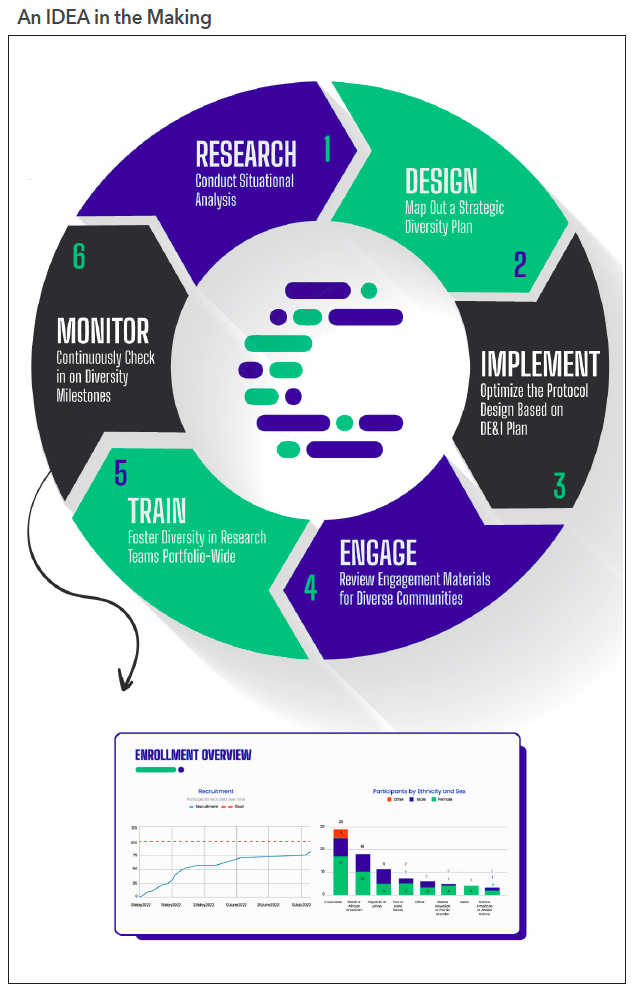






































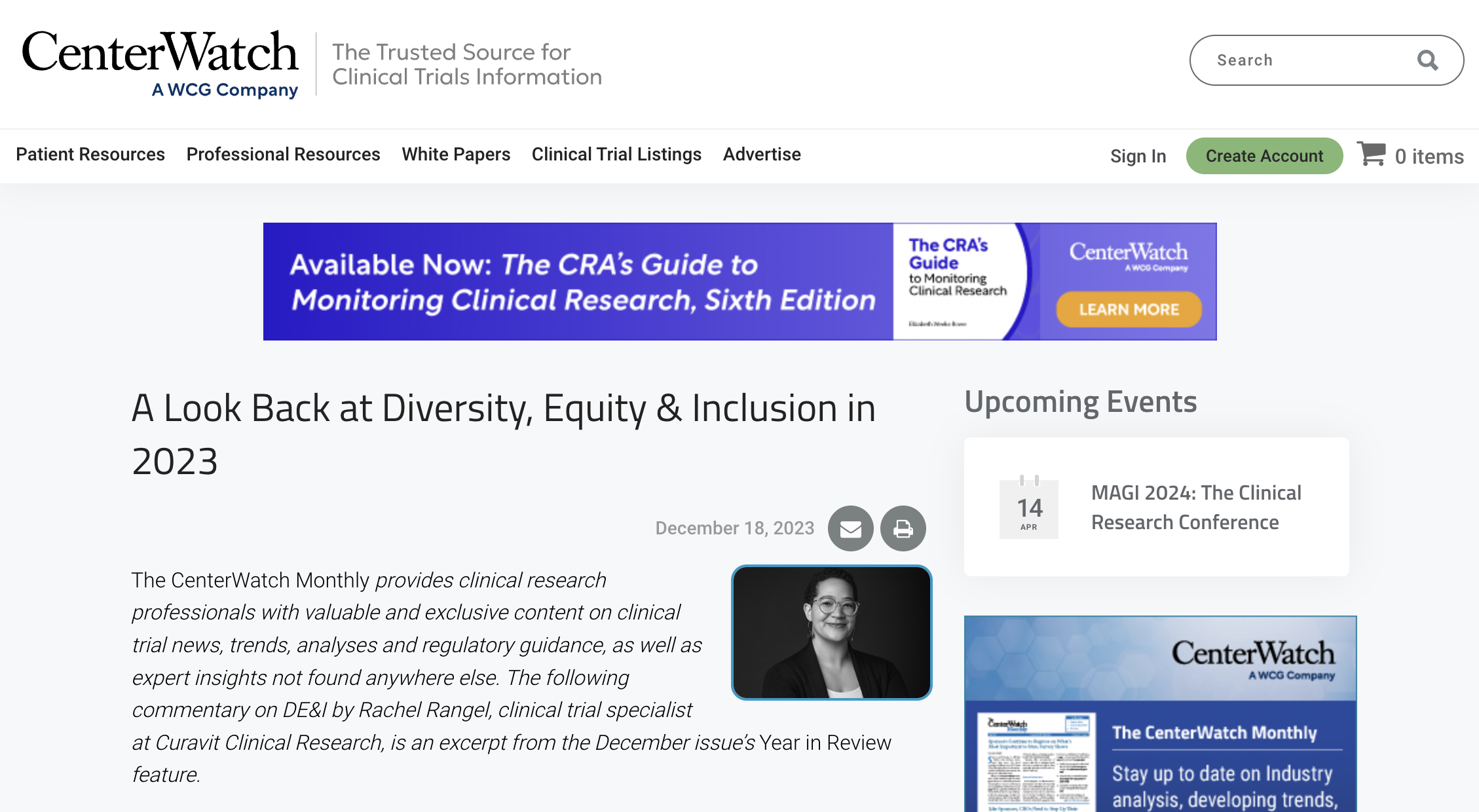


 Joel Morse is founder and CEO of Curavit. He is an experienced operational CEO who has founded, built, and sold large global businesses in healthcare and life sciences. Previously, he founded C3i, a Business Process Outsourcing (BPO) healthcare provider. Morse has a BSc in Mechanical Engineering from Tufts, and an MBA from Columbia.
Joel Morse is founder and CEO of Curavit. He is an experienced operational CEO who has founded, built, and sold large global businesses in healthcare and life sciences. Previously, he founded C3i, a Business Process Outsourcing (BPO) healthcare provider. Morse has a BSc in Mechanical Engineering from Tufts, and an MBA from Columbia. An audiologist by trade, Rachel Rangel has over 10 years of experience as a medical provider. She has served patients across the US — from rural towns to major cities, in small private practices, children’s rehabilitation hospitals, and large medical systems. As the head of Curavit’s Diversity, Equity, & Inclusion initiative, Rangel is working to make clinical trials a more welcoming and inclusive space to those from traditionally underserved and marginalised communities.
An audiologist by trade, Rachel Rangel has over 10 years of experience as a medical provider. She has served patients across the US — from rural towns to major cities, in small private practices, children’s rehabilitation hospitals, and large medical systems. As the head of Curavit’s Diversity, Equity, & Inclusion initiative, Rangel is working to make clinical trials a more welcoming and inclusive space to those from traditionally underserved and marginalised communities.



























 Dr. Pam Diamond is co-founder and chief medical officer of Curavit, a virtual contract research organisation (VCRO) that designs and executes decentralised clinical trials. She is a board-certified, Boston-based otolaryngologist/head and neck surgeon who was affiliated with Harvard Medical School (HMS) and Massachusetts Eye and Ear Infirmary (MEEI) for over 30 years. At Curavit, Dr. Diamond provides medical and scientific expertise and oversight to the design and execution of Curavit’s decentralised clinical trials. She received her medical degree from the University of Rochester School of Medicine and completed her otolaryngology/head and neck surgery residency at Harvard Medical School/MEEI.
Dr. Pam Diamond is co-founder and chief medical officer of Curavit, a virtual contract research organisation (VCRO) that designs and executes decentralised clinical trials. She is a board-certified, Boston-based otolaryngologist/head and neck surgeon who was affiliated with Harvard Medical School (HMS) and Massachusetts Eye and Ear Infirmary (MEEI) for over 30 years. At Curavit, Dr. Diamond provides medical and scientific expertise and oversight to the design and execution of Curavit’s decentralised clinical trials. She received her medical degree from the University of Rochester School of Medicine and completed her otolaryngology/head and neck surgery residency at Harvard Medical School/MEEI.










































{kind=link}
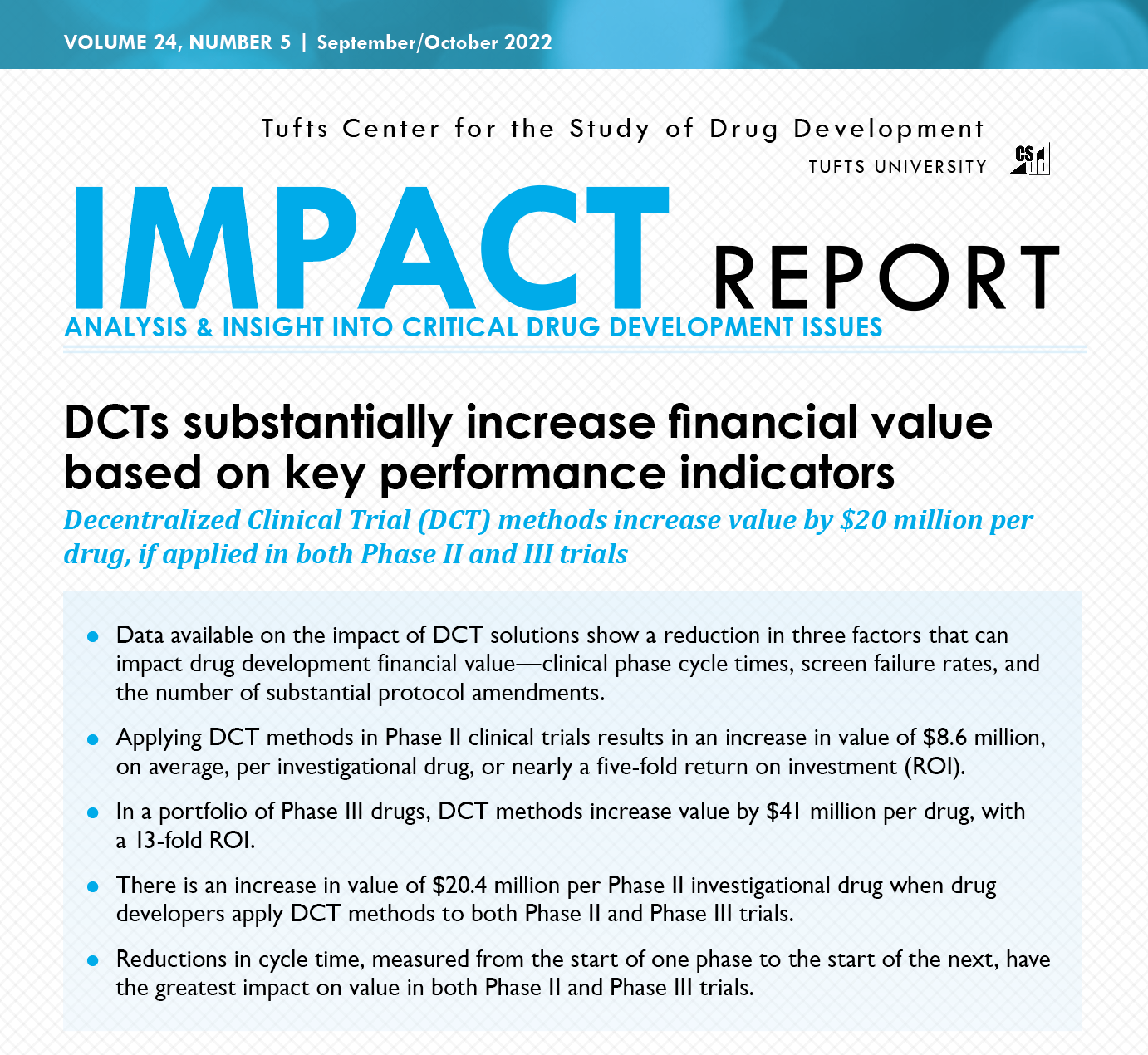{kind=link}